
Cardiac complications — MCQs

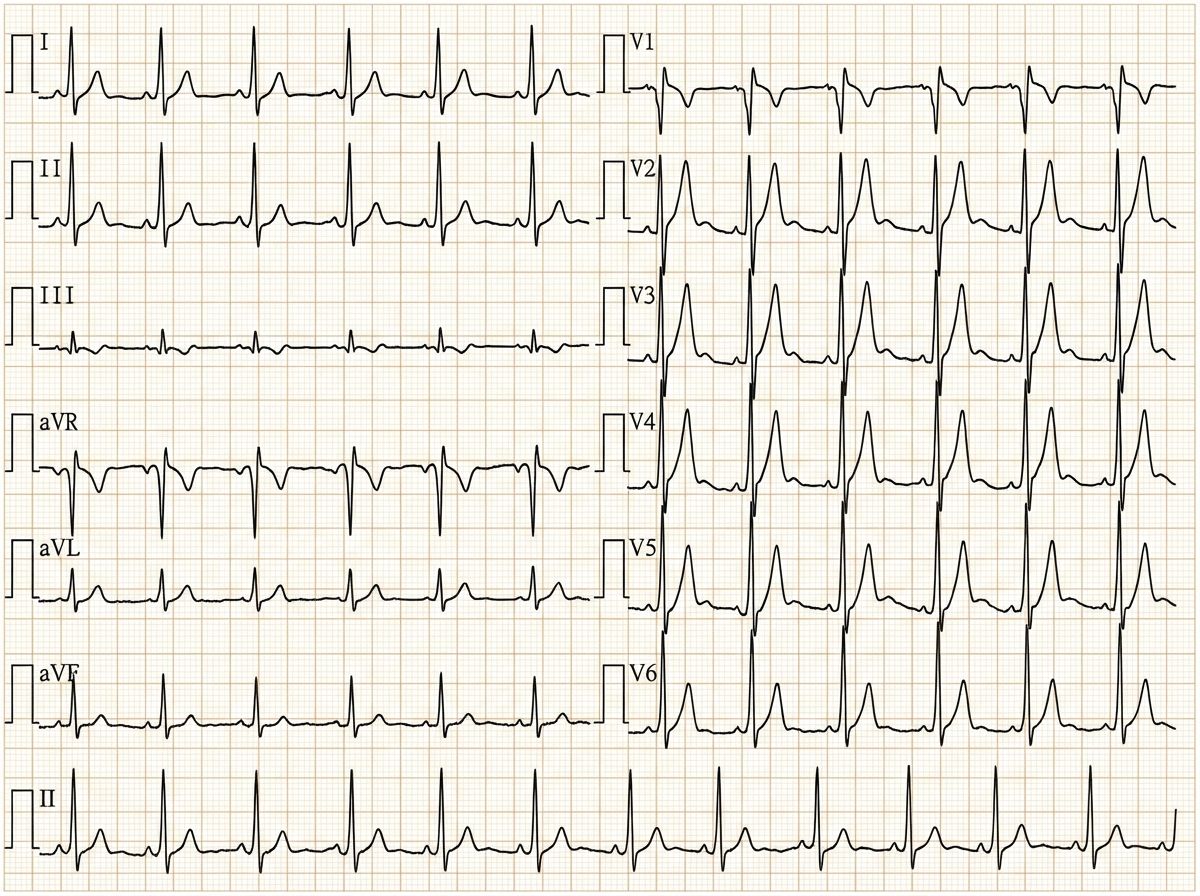
A 29-year-old woman with Wolff-Parkinson-White syndrome presents to her cardiologist’s office for a follow-up visit. She collapsed at her job and made a trip to the emergency department 1 week ago. At that time, she received a diagnosis of atrial fibrillation with rapid ventricular response and hemodynamic instability. While in the emergency department, she underwent direct-current cardioversion to return her heart to sinus rhythm. Her current medications include procainamide. At the cardiologist’s office, her heart rate is 61/min, respiratory rate is 16/min, the temperature is 36.5°C (97.7°F), and blood pressure is 118/60 mm Hg. Her cardiac examination reveals a regular rhythm and a I/VI systolic ejection murmur best heard at the right upper sternal border. An ECG obtained in the clinic is shown. Which of the following is the most appropriate treatment to prevent further episodes of tachyarrhythmia?
A 66-year-old man comes to the emergency department because of a 1-day history of chest pain, palpitations, and dyspnea on exertion. He had a similar episode 3 days ago and was diagnosed with an inferior wall myocardial infarction. He was admitted and a percutaneous transluminal coronary angioplasty was successfully done that day. A fractional flow reserve test during the procedure showed complete resolution of the stenosis. Laboratory tests including serum glucose, lipids, and blood count were within normal limits. He was discharged the day after the procedure on a drug regimen of aspirin, simvastatin, and isosorbide dinitrate. At the time of discharge, he had no chest pain or dyspnea. Presently, his vitals are normal and ECG at rest shows new T-wave inversion. Which of the following is the most reliable test for rapidly establishing the diagnosis in this patient?
A 65-year-old man presents to his primary care physician for a pre-operative evaluation. He is scheduled for cataract surgery in 3 weeks. His past medical history is notable for diabetes, hypertension, and severe osteoarthritis of the right knee. His medications include metformin, hydrochlorothiazide, lisinopril, and aspirin. His surgeon ordered blood work 1 month ago, which showed a hemoglobin of 14.2 g/dL, INR of 1.2, and a hemoglobin A1c of 6.9%. His vital signs at the time of the visit show BP: 130/70 mmHg, Pulse: 80, RR: 12, and T: 37.2 C. He has no current complaints and is eager for his surgery. Which of the following is the most appropriate course of action for this patient at this time?
A 67-year-old man presents to the emergency department for squeezing and substernal chest pain. He states that he was at home eating dinner when his symptoms began. The patient has a past medical history of diabetes, hypertension, and dyslipidemia. He is currently taking atorvastatin, lisinopril, insulin, metformin, metoprolol, and aspirin. Six days ago he underwent percutaneous coronary intervention. His temperature is 99.5°F (37.5°C), blood pressure is 197/118 mmHg, pulse is 120/min, respirations are 17/min, and oxygen saturation is 98% on room air. Physical exam reveals an uncomfortable elderly man who is sweating. An ECG is ordered. Which of the following is the best next step in management for this patient?
A 70-year-old male presents for an annual exam. His past medical history is notable for shortness of breath when he sleeps, and upon exertion. Recently he has experienced dyspnea and lower extremity edema that seems to be worsening. Both of these symptoms have resolved since he was started on several medications and instructed to weigh himself daily. Which of the following is most likely a component of his medical management?
A 59-year-old woman comes to the physician for a 3-month history of progressively worsening shortness of breath on exertion and swelling of her legs. She has a history of breast cancer, which was treated with surgery followed by therapy with doxorubicin and trastuzumab 4 years ago. Cardiac examination shows an S3 gallop; there are no murmurs or rubs. Examination of the lower extremities shows pitting edema below the knees. Echocardiography is most likely to show which of the following sets of changes in this patient? $$$ Ventricular wall thickness %%% Ventricular cavity size %%% Diastolic function %%% Aorto-ventricular pressure gradient $$$
A 72-year-old female presents to the emergency department following a syncopal episode while walking down several flights of stairs. The patient has not seen a doctor in several years and does not take any medications. Your work-up demonstrates that she has symptoms of angina and congestive heart failure. Temperature is 36.8 degrees Celsius, blood pressure is 160/80 mmHg, heart rate is 81/min, and respiratory rate is 20/min. Physical examination is notable for a 3/6 crescendo-decrescendo systolic murmur present at the right upper sternal border with radiation to the carotid arteries. Random blood glucose is 205 mg/dL. Which of the following portends the worst prognosis in this patient?
A 60-year-old man presents to the emergency department with progressive dyspnea for the last 3 weeks. He complains of shortness of breath while lying flat and reports nighttime awakenings due to shortness of breath for the same duration. The patient has been a smoker for the last 30 years. Past medical history is significant for myocardial infarction 7 months ago. Current medications include metoprolol, aspirin, and rosuvastatin, but the patient is noncompliant with his medications. His temperature is 37.2°C (98.9°F), the blood pressure is 150/115 mm Hg, the pulse is 110/min, and the respiratory rate is 24/min. Oxygen saturation on room air is 88%. Chest auscultation reveals bilateral crackles and an S3 gallop. On physical examination, the cardiac apex is palpated in left 6th intercostal space. Bilateral pitting edema is present, and the patient is in moderate distress. Which of the following is the best next step in the management of the patient?
A 62-year-old woman presents to the emergency department complaining of fever, worsening fatigue, and muscle weakness for the previous 48 hours. The patient describes her muscle weakness as symmetric and worse in the upper limbs. Her past medical history is significant for long-standing diabetes type 2 complicated by stage 5 chronic kidney disease (CKD) on hemodialysis. She takes lisinopril, verapamil, metformin, and glargine. Today, the patient’s vital signs include: temperature 38.6°C (101.5°F), pulse 80/min, blood pressure 155/89 mm Hg, respirations 24/min, and 95% oxygen saturation on room air. The cardiac and pulmonary exams are unremarkable. The abdomen is soft and non-tender. Her strength is 3/5 in the upper extremities and 4/5 in the lower extremities and her sensation is intact. Deep tendon reflexes are absent in both the upper and lower limbs. A 12-lead electrocardiogram (ECG) is shown in the image below. Blood work is drawn and the patient is admitted and started on continuous cardiac monitoring. Based on the available information, what is the next best step in managing this patient?
A 55-year-old man presents to his primary care physician for a wellness checkup. The patient has a past medical history of alcohol abuse and is currently attending alcoholics anonymous with little success. He is currently drinking roughly 1L of hard alcohol every day and does not take his disulfiram anymore. Which of the following findings is most likely to also be found in this patient?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app