
Pulmonary risk evaluation — MCQs

A 63-year-old man presents to the emergency department because of progressive difficulty with breathing. He has a history of diabetes, hypertension, and chronic bronchitis. He has been receiving medications to moderate his conditions and reports being compliant with his schedule. He reports a recent difficulty with tackling simple chores in the house. He has not been able to walk for more than 1 block over the past few days. His persistent cough has also been worsening with more formation of sputum. During his diagnosis of bronchitis, about a year ago, he had a 40-pack-year smoking history. The patient is in evident distress and uses his accessory muscles to breathe. The vital signs include: temperature 38.6°C (101.5°F), blood pressure 120/85 mm Hg, pulse 100/min, respiratory rate 26/min, and oxygen (O2) saturation 87%. A decrease in breathing sounds with expiratory wheezes is heard on auscultation of the lungs. The arterial blood gas (ABG) analysis shows: PCO2 60 mm Hg PO2 45 mm Hg pH 7.3 HCO3– 25 mEq/L Which of the following is the most appropriate next step in the treatment?
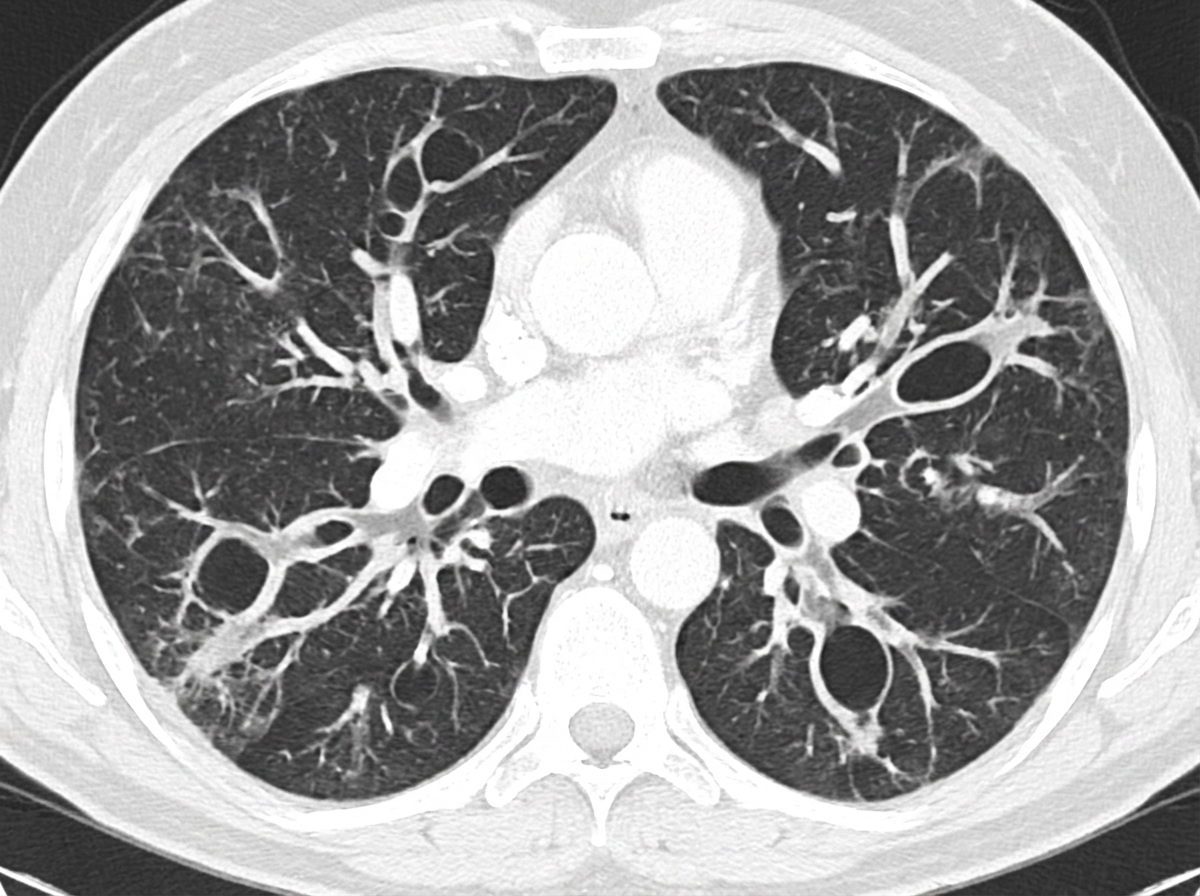
A 47-year-old man comes to the physician because of a 7-week history of cough, shortness of breath, and daily copious sputum production. He has had frequent respiratory tract infections over the past several years. Current medications include dextromethorphan and guaifenesin as needed. He does not smoke cigarettes. His temperature is 37.1°C (98.8°F), pulse is 88/min, respirations are 21/min, and blood pressure is 133/84 mm Hg. Pulse oximetry on room air shows an oxygen saturation of 95%. Diffuse crackles and wheezing are heard on auscultation over bilateral lung fields. A CT scan of the chest is shown. The patient is at greatest risk for which of the following complications?
A 70-year-old man presents to a physician with a cough and difficulty breathing during the last 7 years. He has smoked since his teenage years and regularly inhales tiotropium, formoterol, and budesonide and takes oral theophylline. The number of exacerbations has been increasing over the last 6 months. His temperature is 37.2°C (99°F), the heart rate is 92/min, the blood pressure is 134/88 mm Hg and the respiratory rate is 26/min. On chest auscultation breath sounds are diffusely decreased and bilateral rhonchi are present. Pulse oximetry shows his resting oxygen saturation to be 88%. Chest radiogram shows a flattened diaphragm, hyperlucency of the lungs, and a long, narrow heart shadow. The physician explains this condition to the patient and emphasizes the importance of smoking cessation. In addition to this, which of the following is most likely to reduce the risk of mortality from the condition?
A 75-year-old Caucasian man presents to the emergency department with abdominal pain. The patient states he was at home eating dinner when he began to experience severe abdominal pain. The patient has a past medical history of diabetes, hypertension, and atherosclerosis. He lives at home alone, smokes cigarettes, and drinks 1 to 2 alcoholic drinks per day. The patient is given IV morphine and an ultrasound is obtained demonstrating a dilated abdominal aorta. The patient states that his father died of a similar finding and is concerned about his prognosis. Which of the following is the greatest risk factor for this patient's presentation?
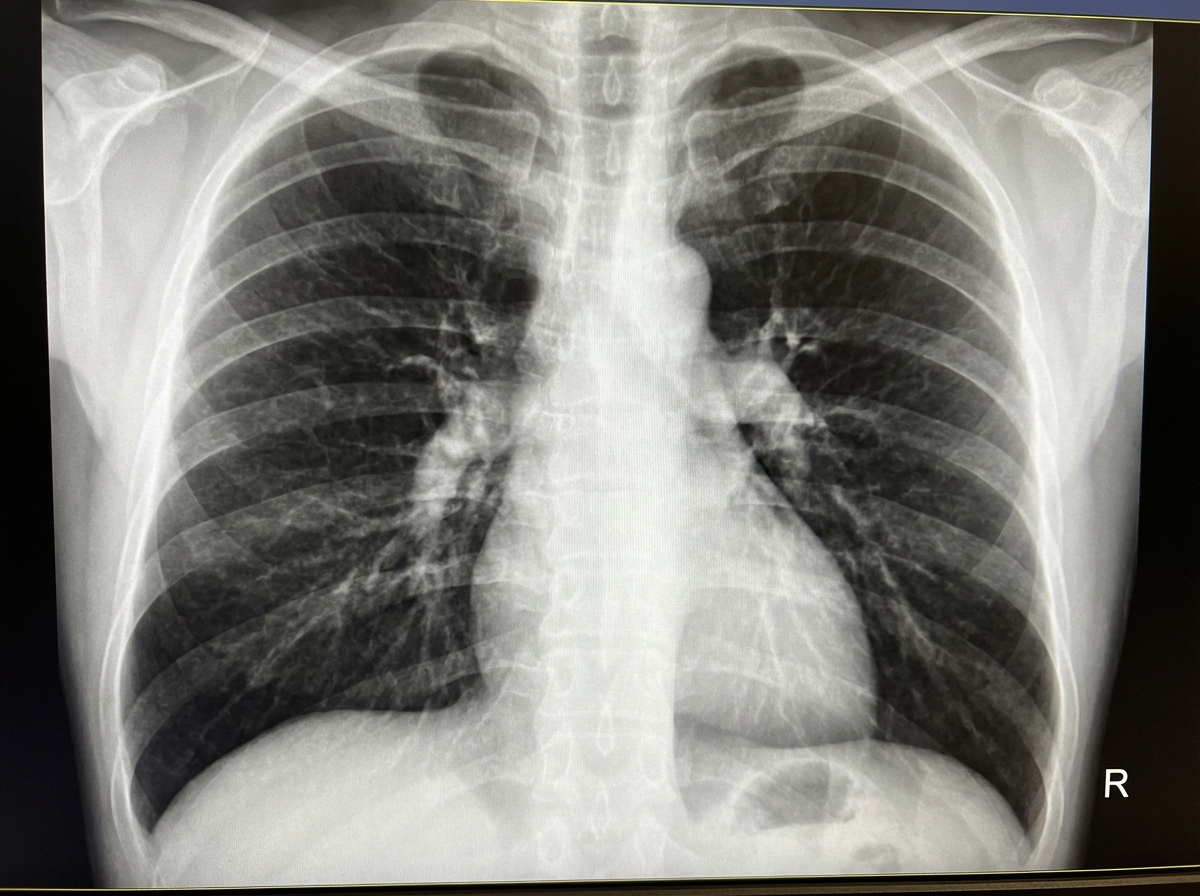
A 68-year-old man presents with shortness of breath, particularly when walking up stairs and when lying down to go to sleep at night. He also complains of a chronic cough and states that he now uses 2 extra pillows at night. The patient has a history of type 2 diabetes that is well-managed with metformin. He also takes Prozac for a long-standing history of depression. The patient has a 60-pack-year smoking history. He also has a history significant for alcohol abuse, but he quit cold turkey 15 years ago when his brother was killed in a drunk driving accident. Both he and his brother were adopted, and he does not know other members of his biological family. Despite repeated efforts of patient counseling, the patient is not interested in quitting smoking. The physical exam is significant for an obese male using accessory muscles of respiration. The vital signs include: temperature 36.8°C (98.2°F), heart rate 95/min, respiratory rate 16/min, and blood pressure 130/85 mm Hg. The oxygen saturation is 90% on room air. Additional physical exam findings include cyanotic lips, peripheral edema, hepatomegaly, and ascites. The cardiovascular exam is significant for an S3 heart sound and elevated JVP. The pulmonary exam is significant for expiratory wheezing, diffuse rhonchi, and hyperresonance on percussion. The laboratory test results are as follows: BUN 15 mg/dL pCO2 60 mm Hg Bicarbonate (HCO3) 32 mmol/L Creatinine 0.8 mg/dL Glucose 95 mg/dL Serum chloride 103 mmol/L Serum potassium 3.9 mEq/L Serum sodium 140 mEq/L Total calcium 2.3 mmol/L Hemoglobin 26 g/dL Bilirubin total 0.9 mg/dL Bilirubin indirect 0.4 mg/dL Iron 100 Ferritin 70 TIBC 300 The posterior-anterior chest X-ray is shown in the image. Which of the following interventions is indicated for decreasing the mortality of this patient?
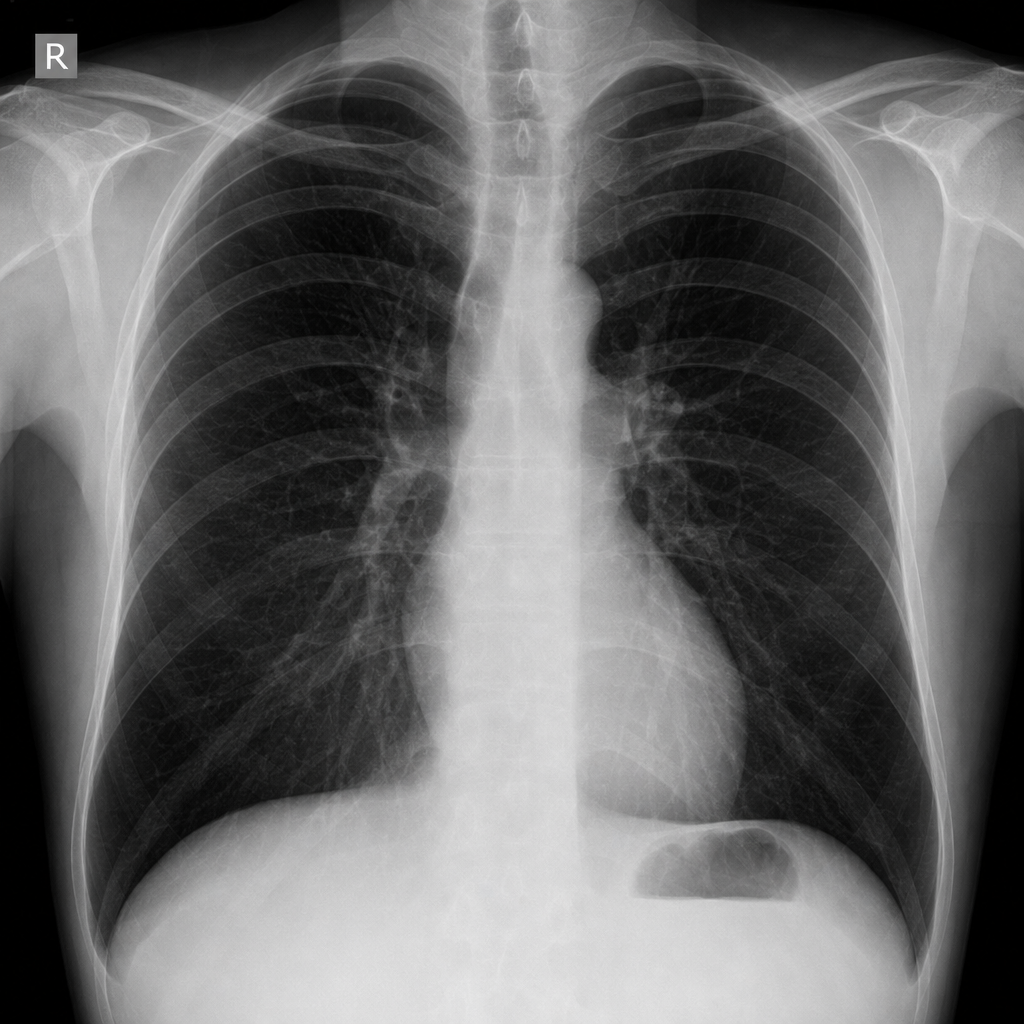
A 55-year-old man with a 60 pack-year smoking history is referred by his primary care physician for a pulmonary function test (PFT). A previously obtained chest x-ray is shown below. Which of the following will most likely appear in his PFT report?
A 60-year-old man presents to the emergency department complaining of worsening exertional dyspnea over the last week. He denies chest pain and lightheadedness but reports persistent cough with white sputum. His past medical history includes hypertension and diabetes mellitus. He has a 50 pack-year history of smoking but denies any illicit drug use or alcohol consumption. His temperature is 101°F (38.3°C), blood pressure is 154/104 mmHg, pulse is 110/min, respirations are 26/min, and oxygen saturation is 88% on a non-rebreather mask. Physical exam is notable for an obese man in distress. The anteroposterior diameter of the patient's chest is increased, and he has decreased breath sounds bilaterally with diffuse expiratory wheezing. Which of the following is the best next step in management?
A 57-year-old man presents to the clinic for a chronic cough over the past 4 months. The patient reports a productive yellow/green cough that is worse at night. He denies any significant precipitating event prior to his symptoms. He denies fever, chest pain, palpitations, weight changes, or abdominal pain, but endorses some difficulty breathing that waxes and wanes. He denies alcohol usage but endorses a 35 pack-year smoking history. A physical examination demonstrates mild wheezes, bibasilar crackles, and mild clubbing of his fingertips. A pulmonary function test is subsequently ordered, and partial results are shown below: Tidal volume: 500 mL Residual volume: 1700 mL Expiratory reserve volume: 1500 mL Inspiratory reserve volume: 3000 mL What is the functional residual capacity of this patient?
A 45-year-old man with a 15-pack-year smoking history is referred for pulmonary function testing. On physical exam, he appears barrel-chested and mildly overweight, but breathes normally. Which of the following tests will most accurately measure his total lung capacity?
A 35-year-old male presents to the emergency room with difficulty breathing. He is accompanied by his wife who reports that they were eating peanuts while lying in bed on their backs when he suddenly started coughing profusely. He has a significant cough and has some trouble breathing. His past medical history is notable for obesity, obstructive sleep apnea, seasonal allergies, and alcohol abuse. He uses a continuous positive airway pressure machine nightly. His medications include cetirizine and fish oil. He has a 10 pack-year smoking history. His temperature is 98.6°F (37°C), blood pressure is 125/30 mmHg, pulse is 110/min, and respirations are 23/min. Which of the following lung segments is most likely affected in this patient?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app