
Neonatal surgical emergencies — MCQs

A 4-week-old infant is brought to the emergency department by his parents with violent vomiting. It started about 3 days ago and has slowly gotten worse. He vomits after most feedings but seems to keep some formula down. His mother notes that he is eager to feed between episodes and seems to be putting on weight. Other than an uncomplicated course of chlamydia conjunctivitis, the infant has been healthy. He was born at 39 weeks gestation via spontaneous vaginal delivery. He is up to date on all vaccines and is meeting all developmental milestones. The physical exam is significant for a palpable mass in the right upper quadrant. What is the first-line confirmatory diagnostic test and associated finding?
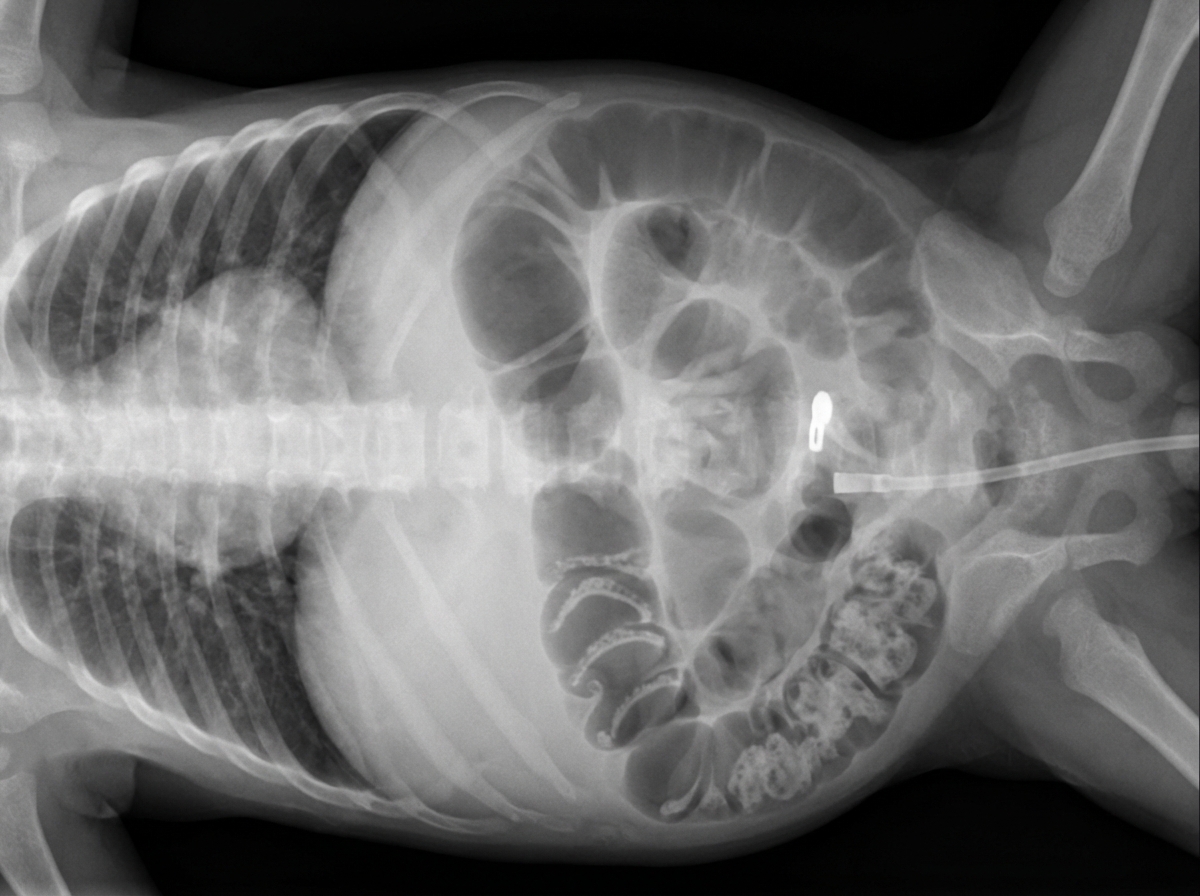
A four-week-old female is evaluated in the neonatal intensive care unit for feeding intolerance with gastric retention of formula. She was born at 25 weeks gestation to a 32-year-old gravida 1 due to preterm premature rupture of membranes at 24 weeks gestation. The patient’s birth weight was 750 g (1 lb 10 oz). She required resuscitation with mechanical ventilation at the time of delivery, but she was subsequently extubated to continuous positive airway pressure (CPAP) and then weaned to nasal cannula. The patient was initially receiving both parenteral nutrition and enteral feeds through a nasogastric tube, but she is now receiving only continuous nasogastric formula feeds. Her feeds are being advanced to a target weight gain of 20-30 g per day. Her current weight is 1,350 g (2 lb 16 oz). The patient’s temperature is 97.2°F (36.2°C), blood pressure is 72/54 mmHg, pulse is 138/min, respirations are 26/min, and SpO2 is 96% on 4L nasal cannula. On physical exam, the patient appears lethargic. Her abdomen is soft and markedly distended. Digital rectal exam reveals stool streaked with blood in the rectal vault. Which of the following abdominal radiographs would most likely be seen in this patient?
A 7-month-old boy is brought to the ED by his mother because of abdominal pain. Two weeks ago, she noticed he had a fever and looser stools, but both resolved after a few days. One week ago, he began to experience periodic episodes during which he would curl up into a ball, scream, and cry. The episodes lasted a few minutes, and were occasionally followed by vomiting. Between events, he was completely normal. She says the episodes have become more frequent over time, and this morning, she noticed blood in his diaper. In the ED, his vitals are within normal ranges, and his physical exam is normal. After confirming the diagnosis with an abdominal ultrasound, what is the next step in management?
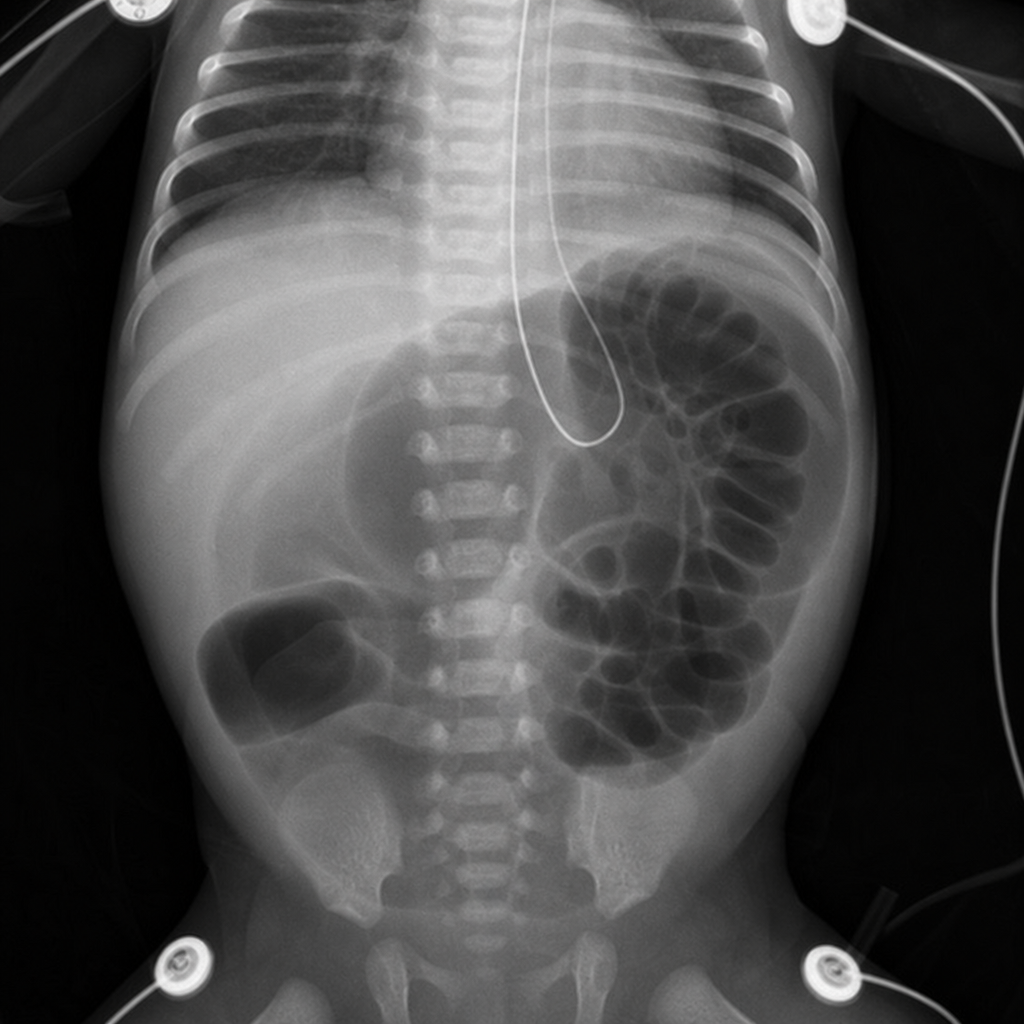
One week after delivery, a 3550-g (7-lb 13-oz) newborn has multiple episodes of bilious vomiting and abdominal distention. He passed urine 14 hours after delivery and had his first bowel movement 3 days after delivery. He was born at term to a 31-year-old woman. Pregnancy was uncomplicated and the mother received adequate prenatal care. His temperature is 37.1°C (98.8°F), pulse is 132/min, and respirations are 50/min. Examination shows a distended abdomen. Bowel sounds are hypoactive. Digital rectal examination shows a patent anus and an empty rectum. The remainder of the examination shows no abnormalities. An x-ray of the abdomen is shown. Which of the following is the underlying cause of these findings?
A 16-year-old man presents to the emergency department with a 2-hour history of sudden-onset abdominal pain. He was playing football when his symptoms started. The patient’s past medical history is notable only for asthma. Social history is notable for unprotected sex with 4 women in the past month. His temperature is 99.3°F (37.4°C), blood pressure is 120/88 mmHg, pulse is 117/min, respirations are 14/min, and oxygen saturation is 99% on room air. Physical exam is noted for a non-tender abdomen. Testicular exam reveals a right testicle which is elevated with a horizontal lie and the scrotum is neither swollen nor discolored. Which of the following is the most likely diagnosis?
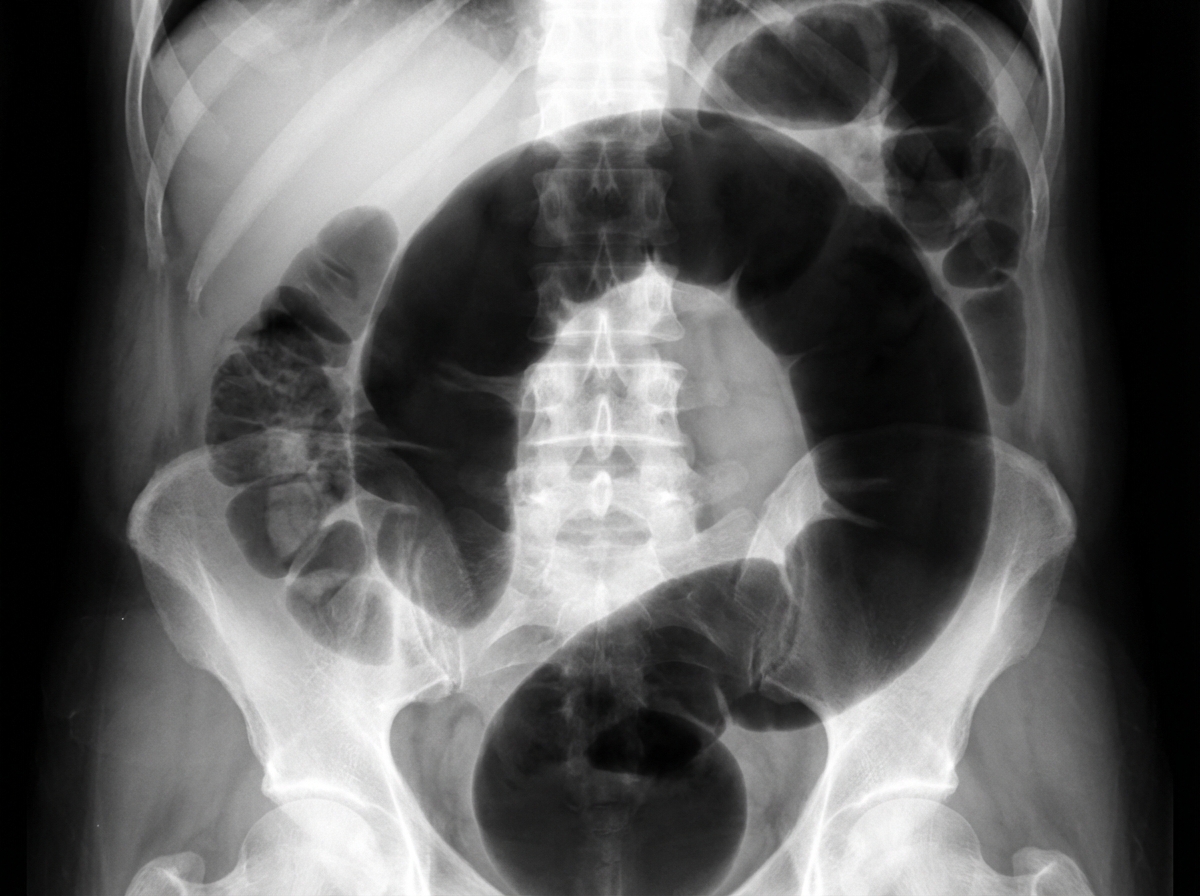
An institutionalized 65-year-old man is brought to the emergency department because of abdominal pain and distension for 12 hours. The pain was acute in onset and is a cramping-type pain associated with nausea, vomiting, and constipation. He has a history of chronic constipation and has used laxatives for years. There is no history of inflammatory bowel disease in his family. He has not been hospitalized recently. There is no recent history of weight loss or change in bowel habits. On physical examination, the patient appears ill. The abdomen is distended with tenderness mainly in the left lower quadrant and is tympanic on percussion. The blood pressure is 110/79 mm Hg, heart rate is 100/min, the respiratory rate is 20/min, and the temperature is 37.2°C (99.0°F). The CBC shows an elevated white blood cell count. The plain abdominal X-ray is shown in the accompanying image. What is the most likely cause of his condition?
A 68-year-old man is brought to the emergency department because of fever, progressive weakness, and cough for the past five days. He experienced a similar episode 2 months ago, for which he was hospitalized for 10 days while visiting his son in Russia. He states that he has never fully recovered from that episode. He felt much better after being treated with antibiotics, but he still coughs often during meals. He sometimes also coughs up undigested food after eating. For the last 5 days, his coughing has become more frequent and productive of yellowish-green sputum. He takes hydrochlorothiazide for hypertension and pantoprazole for the retrosternal discomfort that he often experiences while eating. He has smoked half a pack of cigarettes daily for the last 30 years and drinks one shot of vodka every day. The patient appears thin. His temperature is 40.1°C (104.2°F), pulse is 118/min, respirations are 22/min, and blood pressure is 125/90 mm Hg. Auscultation of the lungs shows right basal crackles. There is dullness on percussion at the right lung base. The remainder of the physical examination shows no abnormalities. Laboratory studies show: Hemoglobin 15.4 g/dL Leukocyte count 17,000/mm3 Platelet count 350,000/mm3 Na+ 139 mEq/L K+ 4.6 mEq/L Cl- 102 mEq/L HCO3- 25 mEq/L Urea Nitrogen 16 mg/dL Creatinine 1.3 mg/dL An x-ray of the chest shows a right lower lobe infiltrate. Which of the following is the most likely explanation for this patient's symptoms?
A 63-year-old man presents to the ambulatory medical clinic with symptoms of dysphagia and ‘heartburn’, which he states have become more troublesome over the past year. Past medical history is significant for primary hypertension. On physical exam, he is somewhat tender to palpation over his upper abdomen. The vital signs include: temperature 36.7°C (98.0°F), blood pressure 126/74 mm Hg, heart rate 74/min, and respiratory rate 14/min. Barium swallow fluoroscopy demonstrates a subdiaphragmatic gastroesophageal junction, with herniation of the gastric fundus into the left hemithorax. Given the following options, what is the most appropriate next step in the management of this patient’s underlying condition?
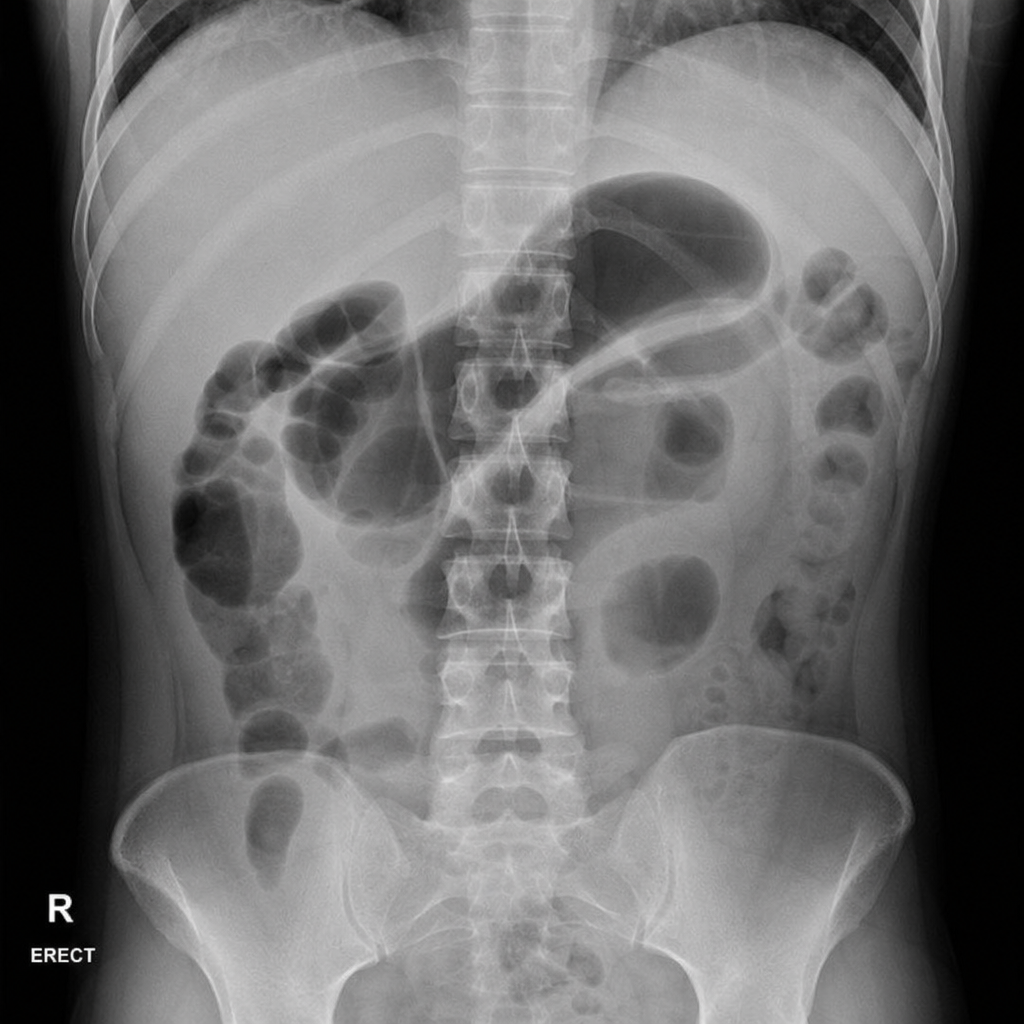
A 45-year-old woman presents to the emergency department with a 12-hour history of severe epigastric pain radiating to the back, nausea, and vomiting. She has a history of gallstones and drinks alcohol occasionally. On examination, she has periumbilical ecchymosis and flank ecchymosis bilaterally. Vital signs: BP 90/60 mmHg, HR 130 bpm, temp 38.1°C, SpO2 94% on 2 L nasal cannula. Serum lipase is 4,200 U/L. A plain abdominal radiograph is obtained. The image demonstrates a gas-filled loop of small bowel in the left upper quadrant with an abrupt transition and absence of gas distally. Which of the following is the most appropriate immediate next step in management?
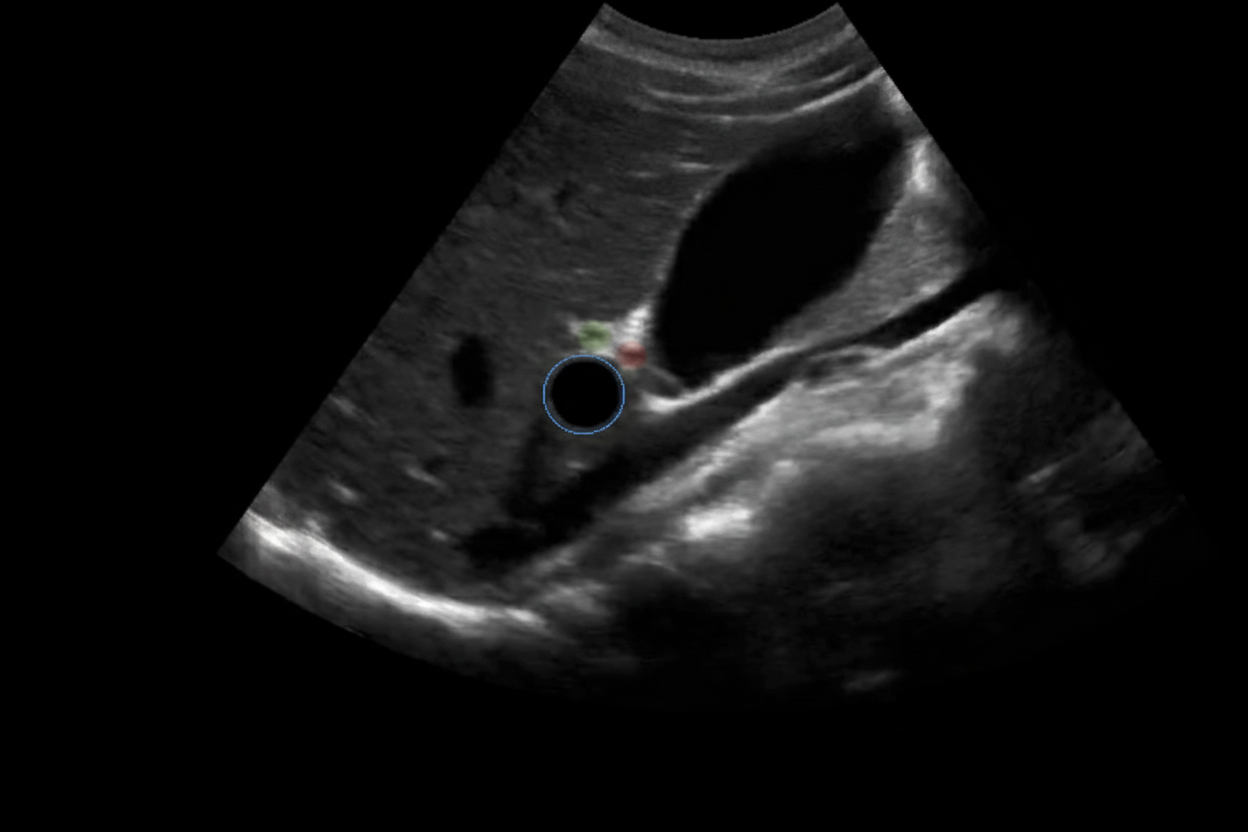
A 6-year-old baby is brought to the hospital by her parents complaining about right upper quadrant pain. On examination the baby is found to have jaundice and palpable abdominal mass. USG of the baby is shown below. What is the most likely cause?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app