
Necrotizing enterocolitis surgical management — MCQs

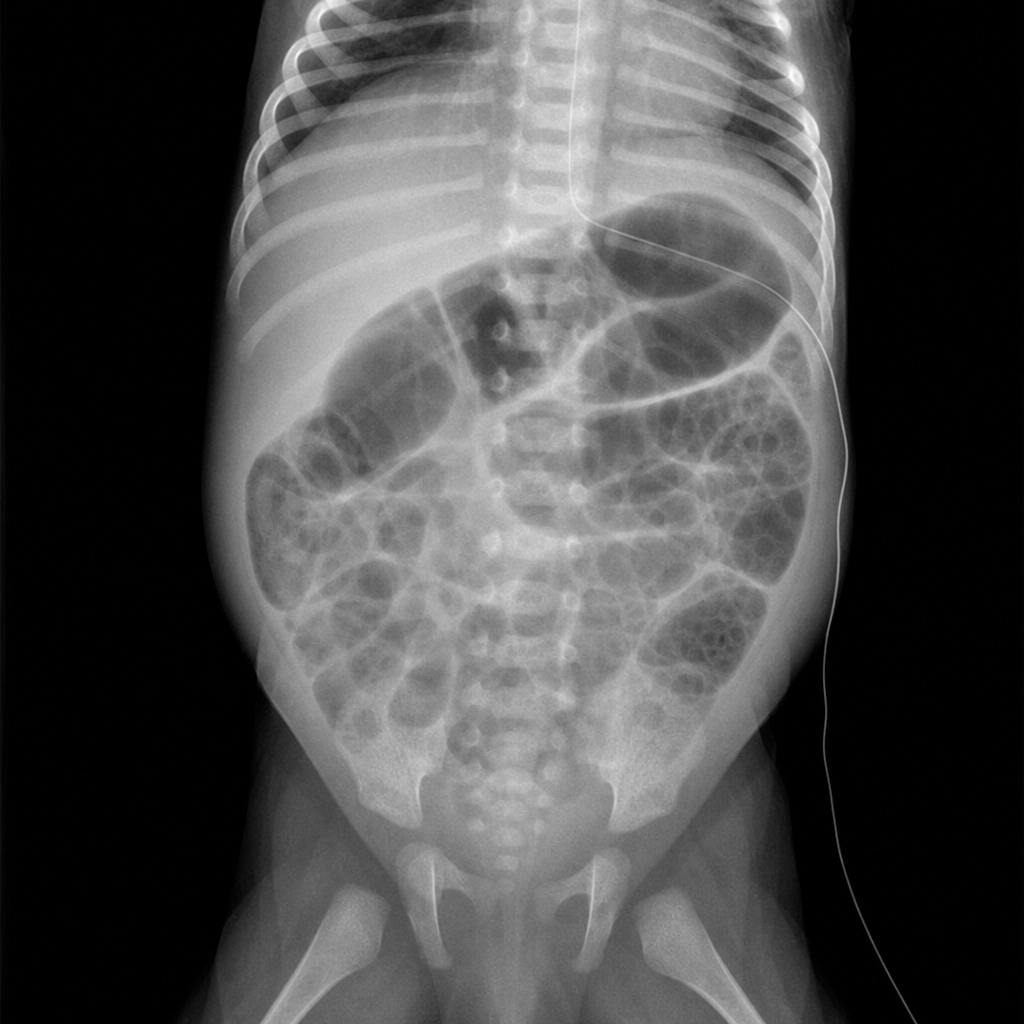
An 18-day-old newborn has difficulty feeding and diarrhea for 2 days. During this period he has vomited after each of his feeds. He was born at 28 weeks' gestation and weighed 1100-g (2-lb 7-oz). His feeds consist of breast milk and cow milk based-formula. He appears lethargic. His temperature is 36.4°C (97.5°F), pulse is 120/min, respirations are 67/min and blood pressure is 70/35 mm Hg. Examination shows diffuse abdominal tenderness; rigidity and guarding are present. Bowel sounds are absent. Test of the stool for occult blood is positive. His hemoglobin concentration is 12.8 g/dL, leukocyte count is 18,000/mm3 and platelet count is 78,000/mm3. An x-ray of the abdomen is shown. Which of the following is the most likely diagnosis?
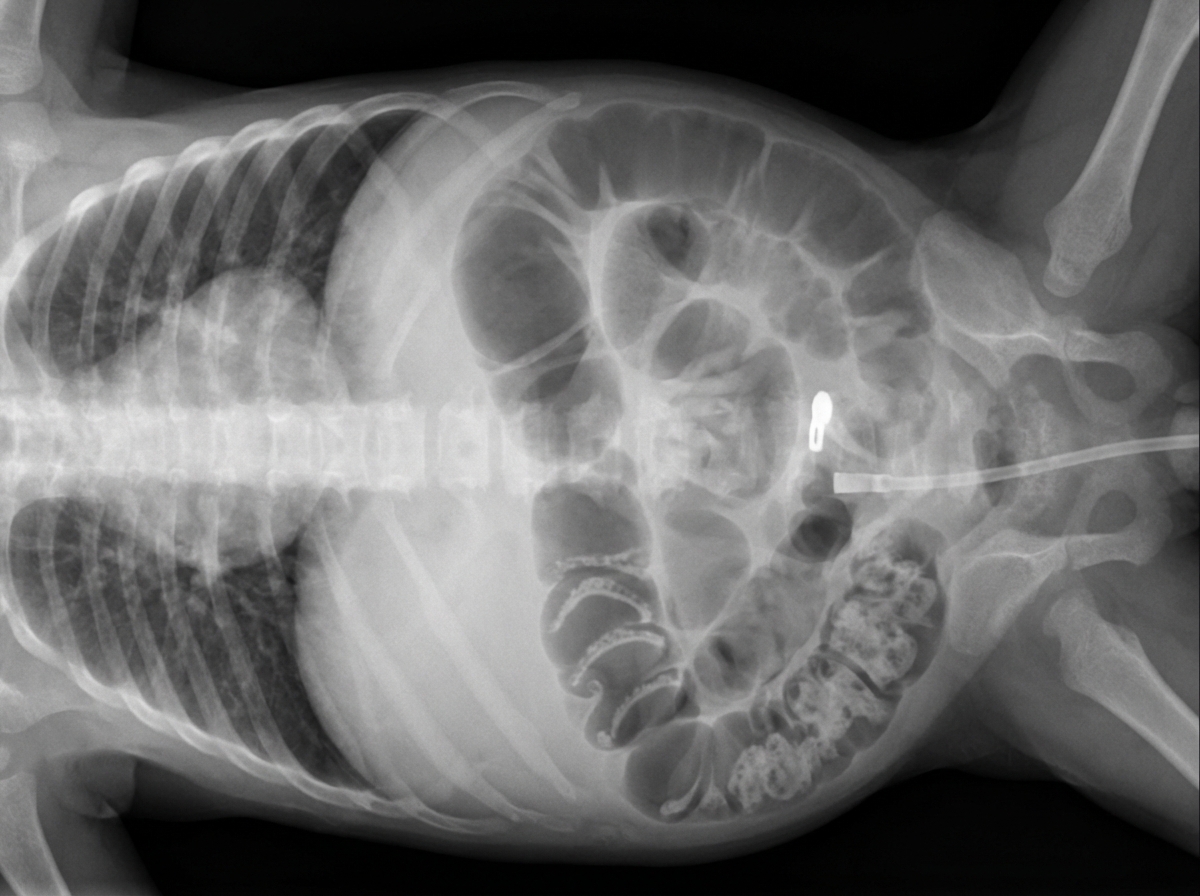
A four-week-old female is evaluated in the neonatal intensive care unit for feeding intolerance with gastric retention of formula. She was born at 25 weeks gestation to a 32-year-old gravida 1 due to preterm premature rupture of membranes at 24 weeks gestation. The patient’s birth weight was 750 g (1 lb 10 oz). She required resuscitation with mechanical ventilation at the time of delivery, but she was subsequently extubated to continuous positive airway pressure (CPAP) and then weaned to nasal cannula. The patient was initially receiving both parenteral nutrition and enteral feeds through a nasogastric tube, but she is now receiving only continuous nasogastric formula feeds. Her feeds are being advanced to a target weight gain of 20-30 g per day. Her current weight is 1,350 g (2 lb 16 oz). The patient’s temperature is 97.2°F (36.2°C), blood pressure is 72/54 mmHg, pulse is 138/min, respirations are 26/min, and SpO2 is 96% on 4L nasal cannula. On physical exam, the patient appears lethargic. Her abdomen is soft and markedly distended. Digital rectal exam reveals stool streaked with blood in the rectal vault. Which of the following abdominal radiographs would most likely be seen in this patient?
A 32-year-old man comes to the emergency department because of recurrent episodes of vomiting for 1 day. He has had over 15 episodes of bilious vomiting. During this period he has had cramping abdominal pain but has not had a bowel movement or passed flatus. He does not have fever or diarrhea. He was diagnosed with Crohn disease at the age of 28 years which has been well controlled with oral mesalamine. He underwent a partial small bowel resection for midgut volvulus at birth. His other medications include vitamin B12, folic acid, loperamide, ferrous sulfate, and vitamin D3. He appears uncomfortable and his lips are parched. His temperature is 37.1°C (99.3°F), pulse is 103/min, and blood pressure is 104/70 mm Hg. The abdomen is distended, tympanitic, and tender to palpation over the periumbilical area and the right lower quadrant. Rectal examination is unremarkable. A CT scan of the abdomen shows multiple dilated loops of small bowel with a transition zone in the mid to distal ileum. After 24 hours of conservative management with IV fluid resuscitation, nasogastric bowel decompression, promethazine, and analgesia, his condition does not improve and a laparotomy is scheduled. During the laparotomy, two discrete strictures are noted in the mid-ileum, around 20 cm apart. Which of the following is the most appropriate next step in management?
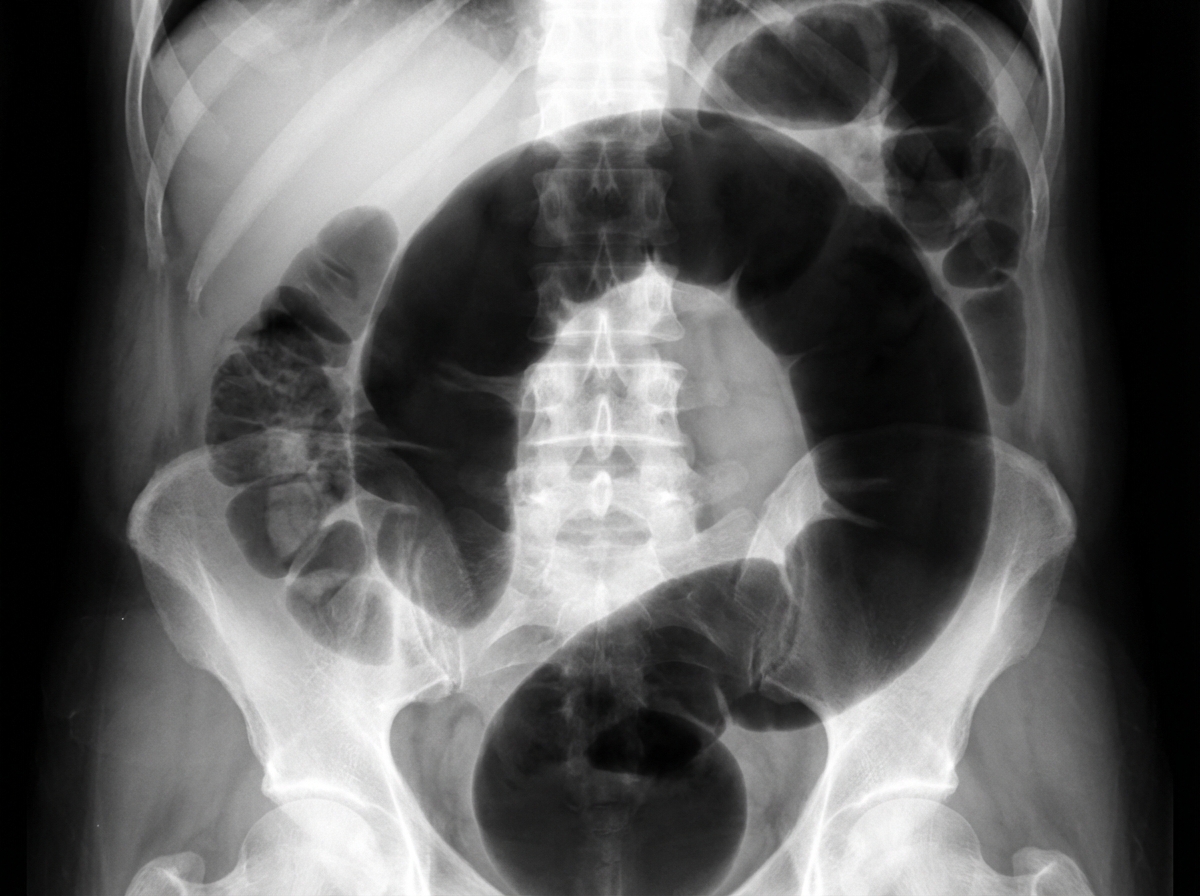
An institutionalized 65-year-old man is brought to the emergency department because of abdominal pain and distension for 12 hours. The pain was acute in onset and is a cramping-type pain associated with nausea, vomiting, and constipation. He has a history of chronic constipation and has used laxatives for years. There is no history of inflammatory bowel disease in his family. He has not been hospitalized recently. There is no recent history of weight loss or change in bowel habits. On physical examination, the patient appears ill. The abdomen is distended with tenderness mainly in the left lower quadrant and is tympanic on percussion. The blood pressure is 110/79 mm Hg, heart rate is 100/min, the respiratory rate is 20/min, and the temperature is 37.2°C (99.0°F). The CBC shows an elevated white blood cell count. The plain abdominal X-ray is shown in the accompanying image. What is the most likely cause of his condition?
A 13-year-old boy is brought to the emergency department by his mother because of vomiting and severe testicular pain for 3 hours. The boy has had 4–5 episodes of vomiting during this period. He has never had a similar episode in the past and takes no medications. His father died of testicular cancer at the age of 50. His immunizations are up-to-date. He appears anxious and uncomfortable. His temperature is 37°C (98.6°F), pulse is 90/min, respirations are 14/min, and blood pressure is 100/60 mm Hg. Cardiopulmonary examination shows no abnormalities The abdomen is soft and nondistended. The left scrotum is firm, erythematous, and swollen. There is severe tenderness on palpation of the scrotum that persists on elevation of the testes. Stroking the inner side of the left thigh fails to elicit elevation of the scrotum. Which of the following is the most appropriate next step in management?
A 27-year-old man is brought to the emergency department by ambulance following a motor vehicle accident 1 hour prior. He appears agitated. His blood pressure is 85/60 mm Hg, the pulse is 110/min, and the respiratory rate is 19/min. Physical examination shows bruising of the left flank and fracture of the left lower thoracic bones. Strict bed rest and monitoring with intravenous fluids is initiated. Urinalysis shows numerous RBCs. A contrast-enhanced CT scan shows normal enhancement of the right kidney. The left renal artery is only visible in the proximal section with a small amount of extravasated blood around the left kidney. The left kidney shows no enhancement. Imaging of the spleen shows no abnormalities. Which of the following is the most appropriate next step in management?
Three days after being admitted to the hospital because of a fall from the roof of a two-story building, a 27-year-old man is being monitored in the intensive care unit. On arrival, the patient was somnolent and not oriented to person, place, or time. A CT scan of the head showed an epidural hemorrhage that was 45 cm3 in size and a midline shift of 7 mm. Emergency surgery was performed with craniotomy and hematoma evacuation on the day of admission. Perioperatively, a bleeding vessel was identified and ligated. Postoperatively, the patient was transferred to the intensive care unit and placed on a ventilator. His temperature is 37°C (98.6°F), pulse is 67/min, and blood pressure is 117/78 mm Hg. The ventilator is set at a FiO2 of 55%, tidal volume of 520 mL, and positive end-expiratory pressure of 5.0 cm H2O. In addition to intravenous administration of fluids, which of the following is the most appropriate next step in managing this patient's nutrition?
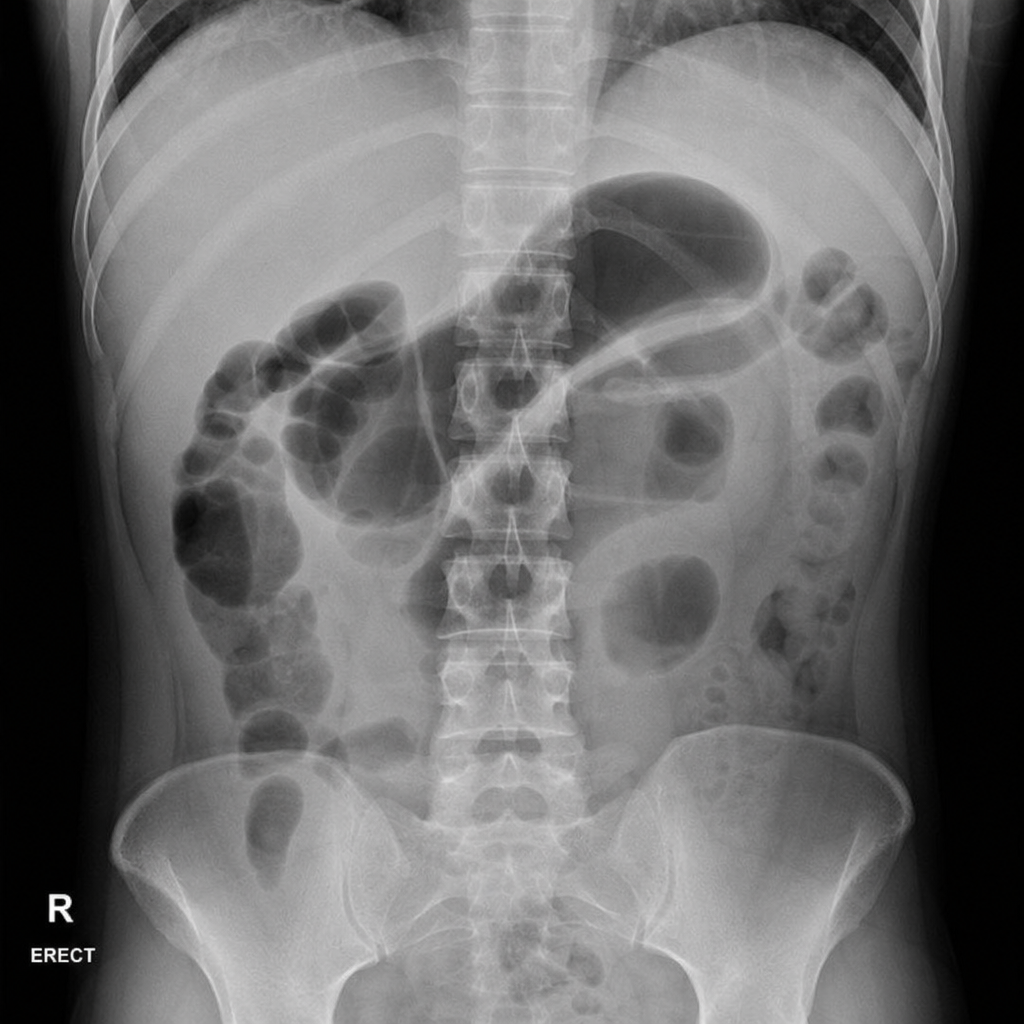
A 45-year-old woman presents to the emergency department with a 12-hour history of severe epigastric pain radiating to the back, nausea, and vomiting. She has a history of gallstones and drinks alcohol occasionally. On examination, she has periumbilical ecchymosis and flank ecchymosis bilaterally. Vital signs: BP 90/60 mmHg, HR 130 bpm, temp 38.1°C, SpO2 94% on 2 L nasal cannula. Serum lipase is 4,200 U/L. A plain abdominal radiograph is obtained. The image demonstrates a gas-filled loop of small bowel in the left upper quadrant with an abrupt transition and absence of gas distally. Which of the following is the most appropriate immediate next step in management?
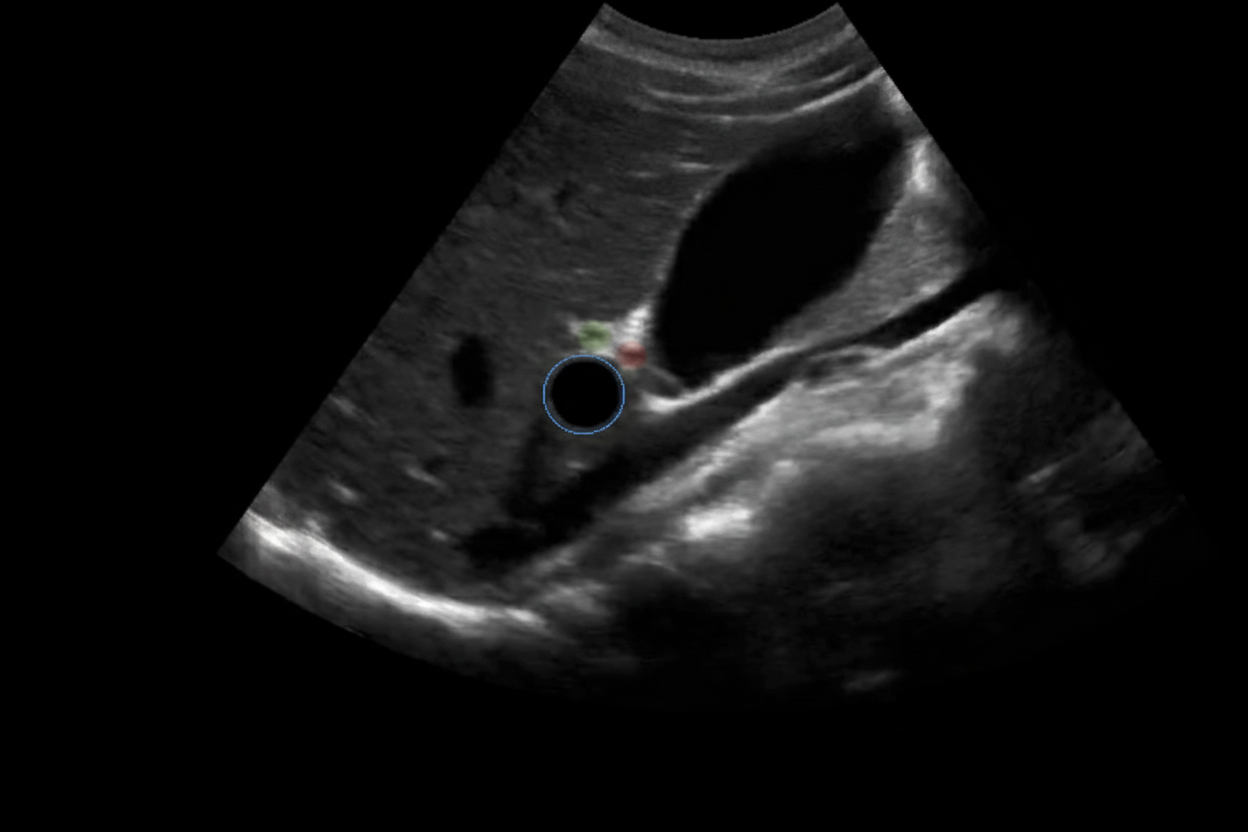
A 6-year-old baby is brought to the hospital by her parents complaining about right upper quadrant pain. On examination the baby is found to have jaundice and palpable abdominal mass. USG of the baby is shown below. What is the most likely cause?
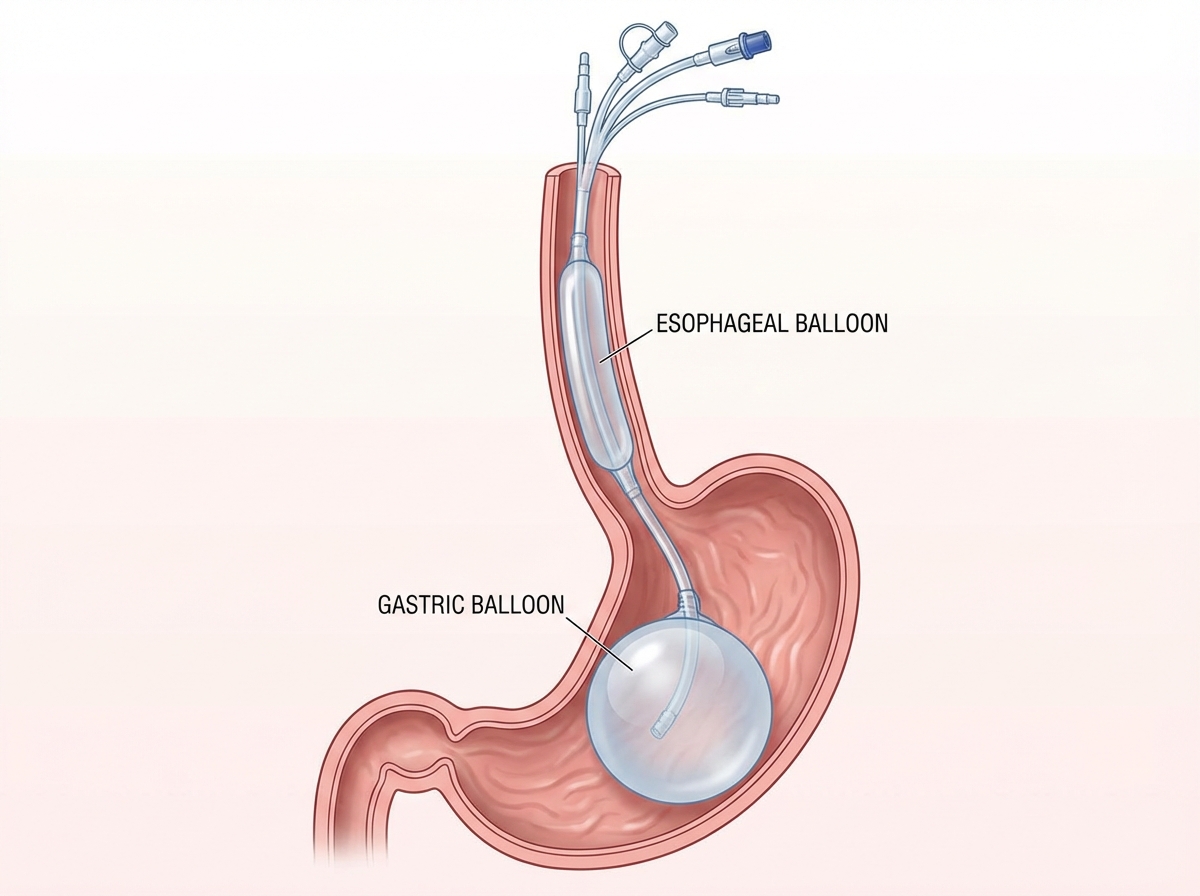
A 12-year-old patient with esophageal varices is managed by the procedure shown in the image. All of the following statements regarding this condition are true except:
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app