
Hirschsprung disease management — MCQs

A 4-month-old girl is brought to the office by her parents because they noticed a mass protruding from her rectum and, she has been producing green colored emesis for the past 24 hours. Her parents noticed the mass when she had a bowel movement while changing her diaper. She strained to have this bowel movement 24 hours ago, shortly afterwards she had 3 episodes of greenish vomiting. She has a past medical history of failure to pass meconium for 2 days after birth. Her vital signs include: heart rate 190/min, respiratory rate 44/min, temperature 37.2°C (99.0°F), and blood pressure 80/50 mm Hg. On physical examination, the abdomen is distended. Examination of the anus reveals extrusion of the rectal mucosa through the external anal sphincter, and digital rectal examination produces an explosive expulsion of gas and stool. The abdominal radiograph shows bowel distention and absence of distal gas. What is the most likely cause?
A 4-week-old infant is brought to the emergency department by his parents with violent vomiting. It started about 3 days ago and has slowly gotten worse. He vomits after most feedings but seems to keep some formula down. His mother notes that he is eager to feed between episodes and seems to be putting on weight. Other than an uncomplicated course of chlamydia conjunctivitis, the infant has been healthy. He was born at 39 weeks gestation via spontaneous vaginal delivery. He is up to date on all vaccines and is meeting all developmental milestones. The physical exam is significant for a palpable mass in the right upper quadrant. What is the first-line confirmatory diagnostic test and associated finding?
A 4-year-old boy is brought to the physician by his parents for bedwetting. He went 3 months without wetting the bed but then started again 6 weeks ago. He has been wetting the bed about 1–2 times per week. He has not had daytime urinary incontinence or dysuria. His teachers report that he is attentive in preschool and plays well with his peers. He is able to name 5 colors, follow three-step commands, and recite his address. He can do a somersault, use scissors, and copy a square. Physical examination shows no abnormalities. Which of the following is the most appropriate next step in management?
A mother brings her 4-year-old boy to the physician, as the boy has a 7-day history of foul-smelling diarrhea, abdominal cramps, and fever. The mother adds that he has been vomiting as well, and she is very much worried. The child is in daycare, and the mother endorses sick contacts with both family and friends. The boy has not been vaccinated as the parents do not think it is necessary. On physical exam, the child appears dehydrated. Stool examination is negative for blood cells, pus, and ova or parasites. What is the most likely diagnosis?
A 2-year-old boy is brought in to his pediatrician for a routine checkup. The parents mention that the child has been developing appropriately, although they have been noticing that the child appears to have chronic constipation. The parents report that their child does not routinely have daily bowel movements, and they have noticed that his abdomen has become more distended recently. In the past, they report that the patient was also delayed in passing meconium, but this was not further worked up. On exam, his temperature is 98.6°F (37.0°C), blood pressure is 110/68 mmHg, pulse is 74/min, and respirations are 14/min. The patient is noted to have a slightly distended abdomen that is nontender. Eventually, this patient undergoes a biopsy. Which of the following layers most likely reveals the causative pathologic finding of this disease?
A 3175-g (7-lb) female newborn is delivered at term. Initial examination shows a distended abdomen and a flat perineal region without an opening. A dark green discharge is coming out of the vulva. Which of the following is the most likely diagnosis?
A 56-year-old woman is one week status post abdominal hysterectomy when she develops a fever of 101.4°F (38.6°C). Her past medical history is significant for type II diabetes mellitus and a prior history of alcohol abuse. The operative report and intraoperative cystoscopy indicate that the surgery was uncomplicated. The nurse reports that since the surgery, the patient has also complained of worsening lower abdominal pain. She has given the patient the appropriate pain medications with little improvement. The patient has tolerated an oral diet well and denies nausea, vomiting, or abdominal distension. Her blood pressure is 110/62 mmHg, pulse is 122/min, and respirations are 14/min. Since being given 1000 mL of intravenous fluids yesterday, the patient has excreted 800 mL of urine. On physical exam, she is uncomfortable, shivering, and sweating. The surgical site is intact, but the surrounding skin appears red. No drainage is appreciated. The abdominal examination reveals tenderness to palpation and hypoactive bowel sounds. Labs and a clean catch urine specimen are obtained as shown below: Leukocyte count and differential: Leukocyte count: 18,000/mm^3 Segmented neutrophils: 80% Bands: 10% Eosinophils: 1% Basophils: < 1% Lymphocytes: 5% Monocytes: 4% Platelet count: 300,000/mm^3 Hemoglobin: 12.5 g/dL Hematocrit: 42% Urine: Epithelial cells: 15/hpf Glucose: positive RBC: 1/hpf WBC: 2/hpf Bacteria: 50 cfu/mL Ketones: none Nitrites: negative Leukocyte esterase: negative Which of the following is most likely the cause of this patient’s symptoms?
A 2-day-old newborn boy has failed to pass meconium after 48 hours. There is an absence of stool in the rectal vault. Family history is significant for MEN2A syndrome. Which of the following confirms the diagnosis?
A 28-year-old male presents to his primary care physician with complaints of intermittent abdominal pain and alternating bouts of constipation and diarrhea. His medical chart is not significant for any past medical problems or prior surgeries. He is not prescribed any current medications. Which of the following questions would be the most useful next question in eliciting further history from this patient?
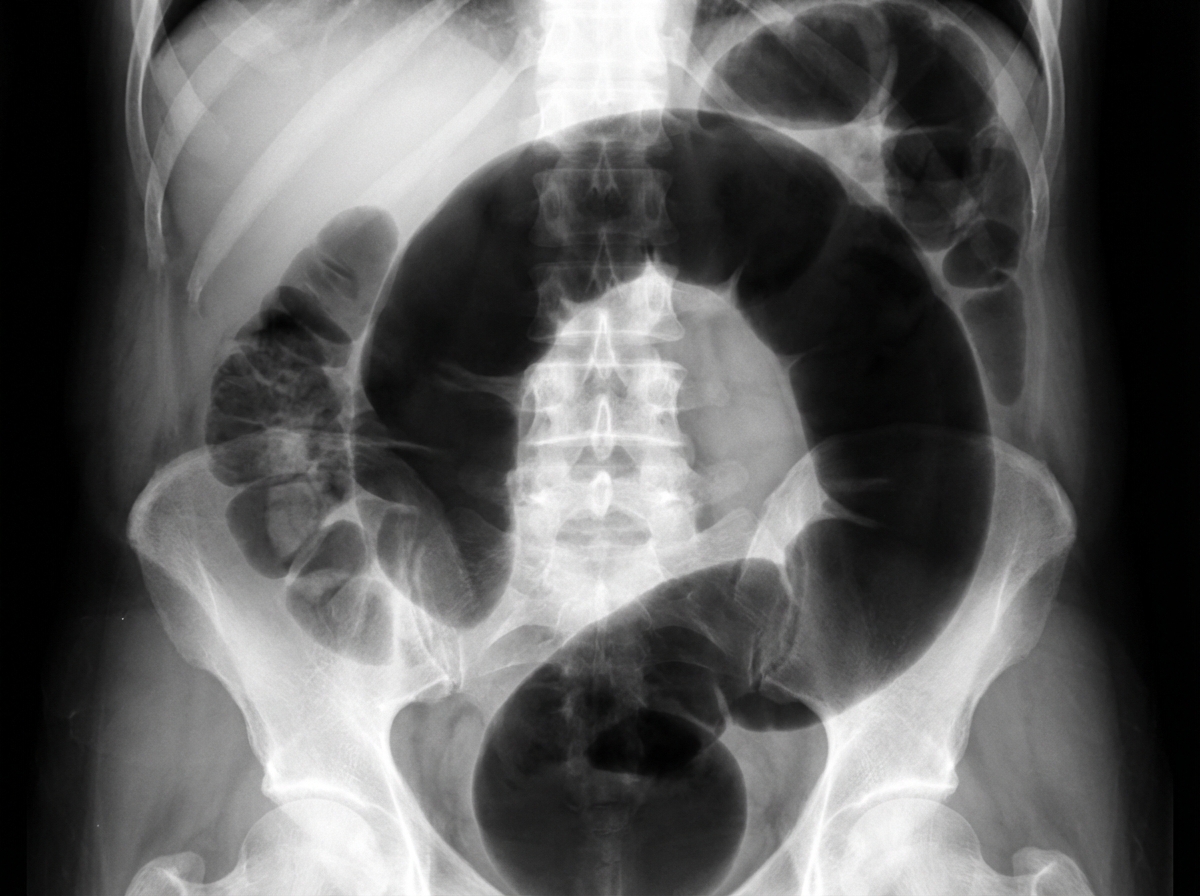
An institutionalized 65-year-old man is brought to the emergency department because of abdominal pain and distension for 12 hours. The pain was acute in onset and is a cramping-type pain associated with nausea, vomiting, and constipation. He has a history of chronic constipation and has used laxatives for years. There is no history of inflammatory bowel disease in his family. He has not been hospitalized recently. There is no recent history of weight loss or change in bowel habits. On physical examination, the patient appears ill. The abdomen is distended with tenderness mainly in the left lower quadrant and is tympanic on percussion. The blood pressure is 110/79 mm Hg, heart rate is 100/min, the respiratory rate is 20/min, and the temperature is 37.2°C (99.0°F). The CBC shows an elevated white blood cell count. The plain abdominal X-ray is shown in the accompanying image. What is the most likely cause of his condition?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app