
Congenital abdominal wall defects — MCQs

A 4-week-old infant is brought to the emergency department by his parents with violent vomiting. It started about 3 days ago and has slowly gotten worse. He vomits after most feedings but seems to keep some formula down. His mother notes that he is eager to feed between episodes and seems to be putting on weight. Other than an uncomplicated course of chlamydia conjunctivitis, the infant has been healthy. He was born at 39 weeks gestation via spontaneous vaginal delivery. He is up to date on all vaccines and is meeting all developmental milestones. The physical exam is significant for a palpable mass in the right upper quadrant. What is the first-line confirmatory diagnostic test and associated finding?
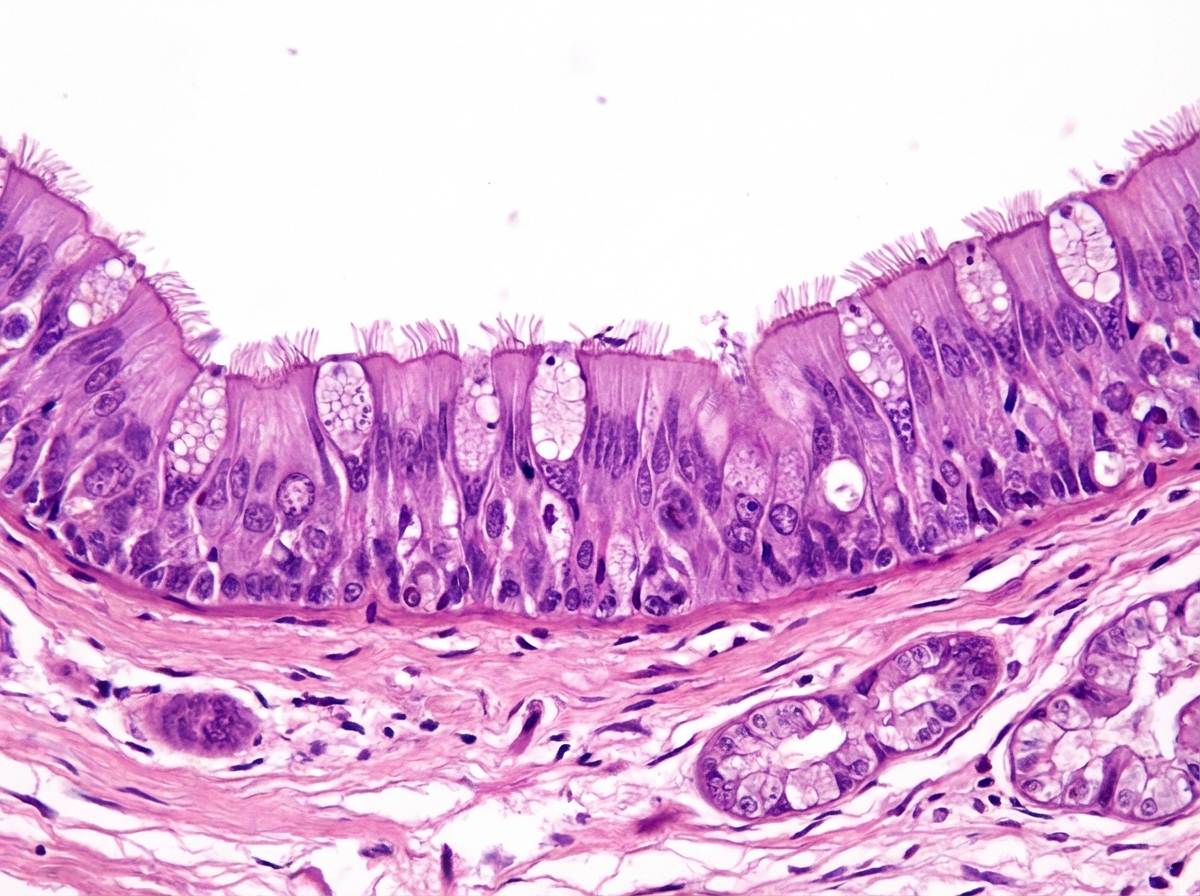
A research team is studying certain congenital anomalies of the respiratory tract. The method consists of marking a certain germinal layer with an isotope, following its development stages in chicken embryos, and finally analyzing the specimen. A given specimen of tissue is presented in the exhibit. Which of the following germinal structures most likely gave rise to the epithelial lining of this specimen?
A 52-year-old man comes to the physician because of a 3-month history of upper abdominal pain and nausea that occurs about 3 hours after eating and at night. These symptoms improve with eating. After eating, he often has a feeling of fullness and bloating. He has had several episodes of dark stools over the past month. He has smoked one pack of cigarettes daily for 40 years and drinks 2 alcoholic beverages daily. He takes no medications. His temperature is 36.4°C (97.5°F), pulse is 80/min, and blood pressure is 110/70 mm Hg. Abdominal examination shows epigastric tenderness with no guarding or rebound. Bowel sounds are normal. Which of the following treatments is most appropriate to prevent further complications of the disease in this patient?
A 4700-g (10.3-lb) male newborn is delivered at 37 weeks' gestation to a 30-year-old woman, gravida 2, para 1. Apgar scores are 7 and 8 at 1 and 5 minutes, respectively. The newborn appears pale. Temperature is 37°C (98.6°F), pulse is 180/min, and blood pressure is 90/60 mm Hg. Examination in the delivery room shows midfacial hypoplasia, infraorbital creases, and a large tongue. The right side of the body is larger than the left. Abdominal examination shows that the abdominal viscera protrudes through the abdominal wall at the umbilicus; the viscera are covered by the amniotic membrane and the peritoneum. The liver is palpated 2–3 cm below the right costal margin. Fingerstick blood glucose concentration is 60 mg/dL. Ultrasonography of the abdomen shows enlarged kidneys bilaterally. In addition to surgical closure of the abdominal wall, which of the following is the most appropriate next step in management?
A 19-year-old woman, gravida 1, para 0, at 21 weeks’ gestation comes to the physician for a follow-up prenatal visit. At her previous appointment, her serum α-fetoprotein concentration was elevated. She had smoked 1 pack of cigarettes daily for 3 years but quit at 6 weeks' gestation. Examination shows a uterus consistent in size with a 21-week gestation. Ultrasonography shows fetal viscera suspended freely into the amniotic cavity. Which of the following is the most likely diagnosis?

A 28-year-old male presents to his primary care physician with complaints of intermittent abdominal pain and alternating bouts of constipation and diarrhea. His medical chart is not significant for any past medical problems or prior surgeries. He is not prescribed any current medications. Which of the following questions would be the most useful next question in eliciting further history from this patient?
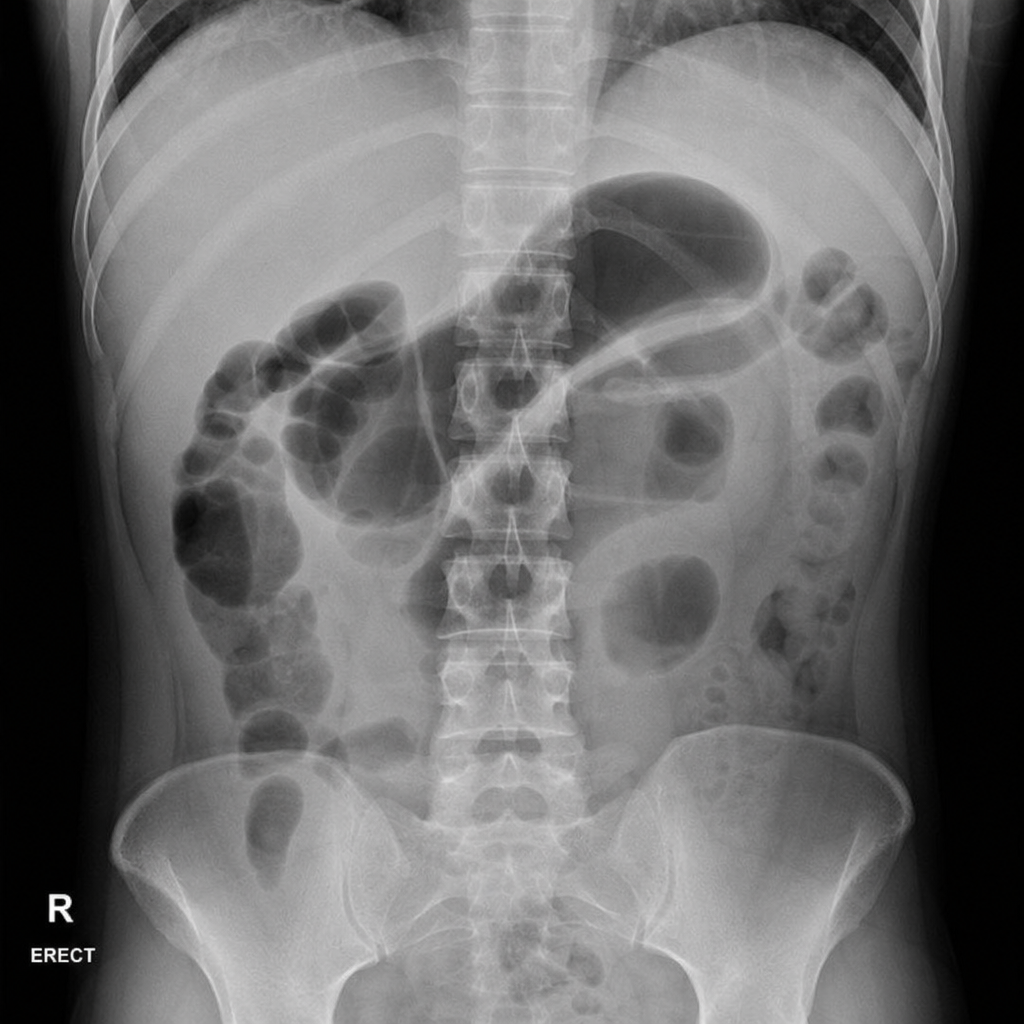
A 45-year-old woman presents to the emergency department with a 12-hour history of severe epigastric pain radiating to the back, nausea, and vomiting. She has a history of gallstones and drinks alcohol occasionally. On examination, she has periumbilical ecchymosis and flank ecchymosis bilaterally. Vital signs: BP 90/60 mmHg, HR 130 bpm, temp 38.1°C, SpO2 94% on 2 L nasal cannula. Serum lipase is 4,200 U/L. A plain abdominal radiograph is obtained. The image demonstrates a gas-filled loop of small bowel in the left upper quadrant with an abrupt transition and absence of gas distally. Which of the following is the most appropriate immediate next step in management?
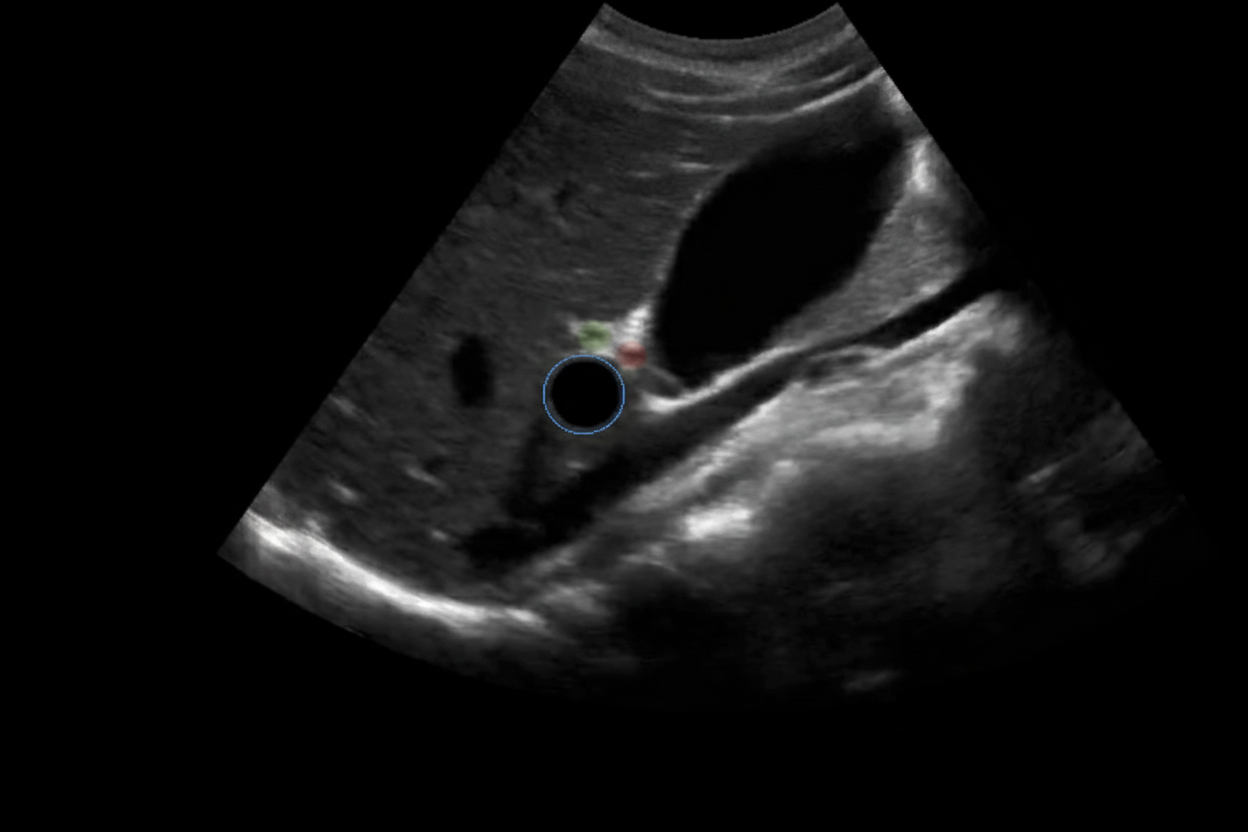
A 6-year-old baby is brought to the hospital by her parents complaining about right upper quadrant pain. On examination the baby is found to have jaundice and palpable abdominal mass. USG of the baby is shown below. What is the most likely cause?
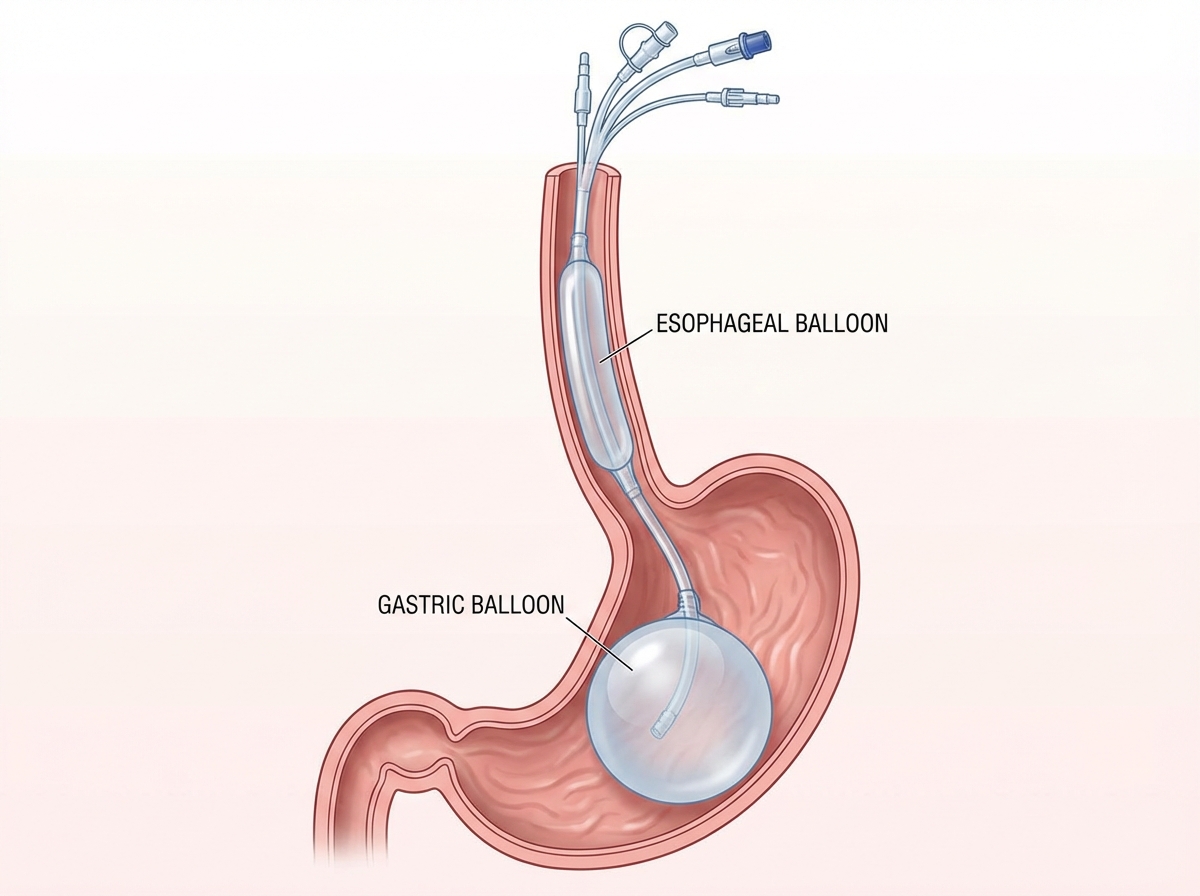
A 12-year-old patient with esophageal varices is managed by the procedure shown in the image. All of the following statements regarding this condition are true except:
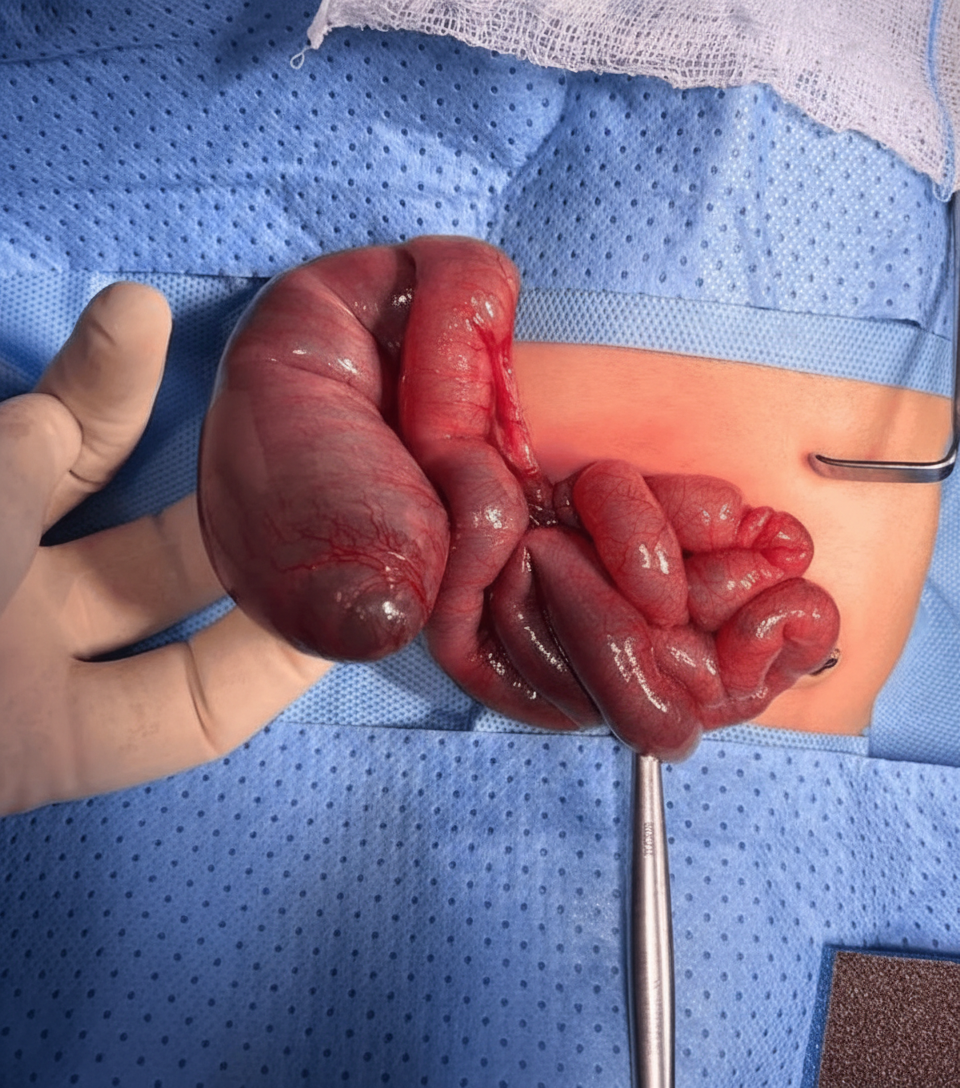
What does the intraoperative image shown below depict?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app