
Pediatric Surgery — MCQs

On this page
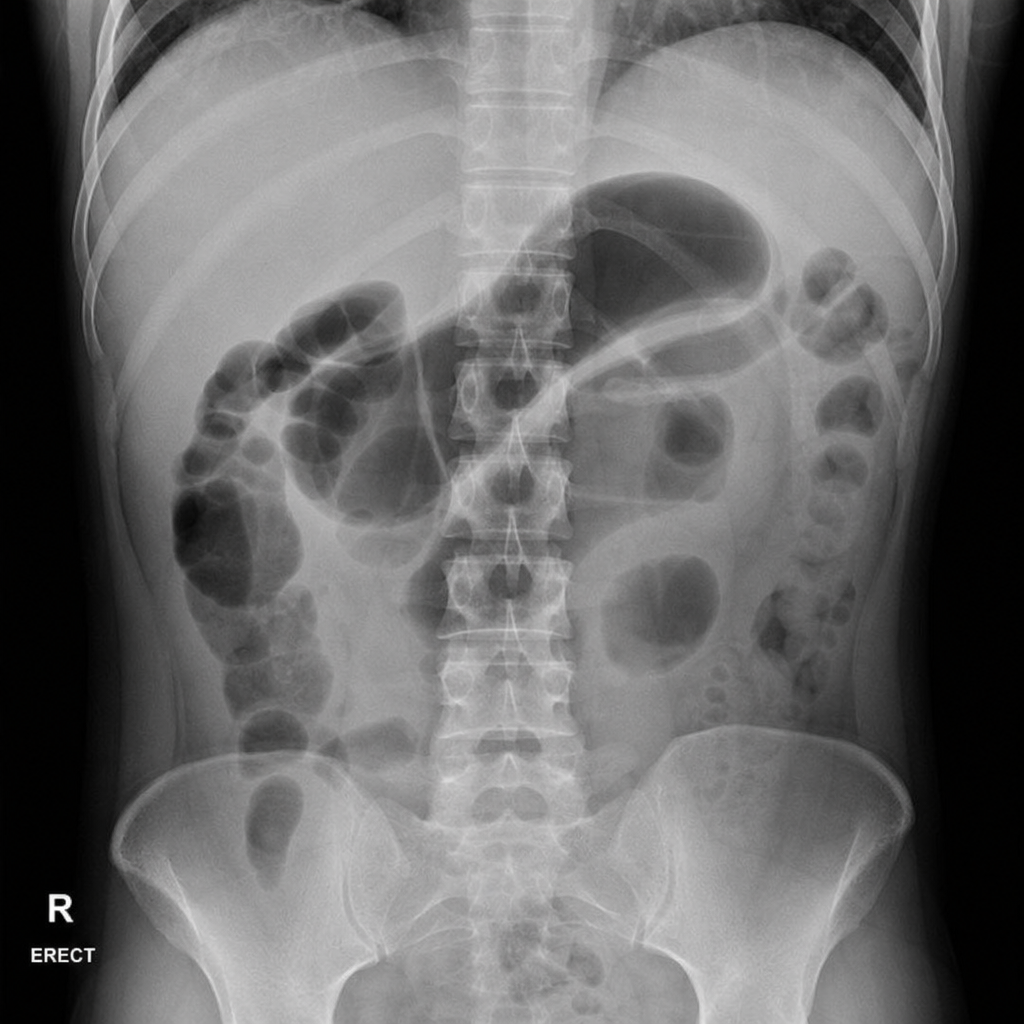
A 45-year-old woman presents to the emergency department with a 12-hour history of severe epigastric pain radiating to the back, nausea, and vomiting. She has a history of gallstones and drinks alcohol occasionally. On examination, she has periumbilical ecchymosis and flank ecchymosis bilaterally. Vital signs: BP 90/60 mmHg, HR 130 bpm, temp 38.1°C, SpO2 94% on 2 L nasal cannula. Serum lipase is 4,200 U/L. A plain abdominal radiograph is obtained. The image demonstrates a gas-filled loop of small bowel in the left upper quadrant with an abrupt transition and absence of gas distally. Which of the following is the most appropriate immediate next step in management?
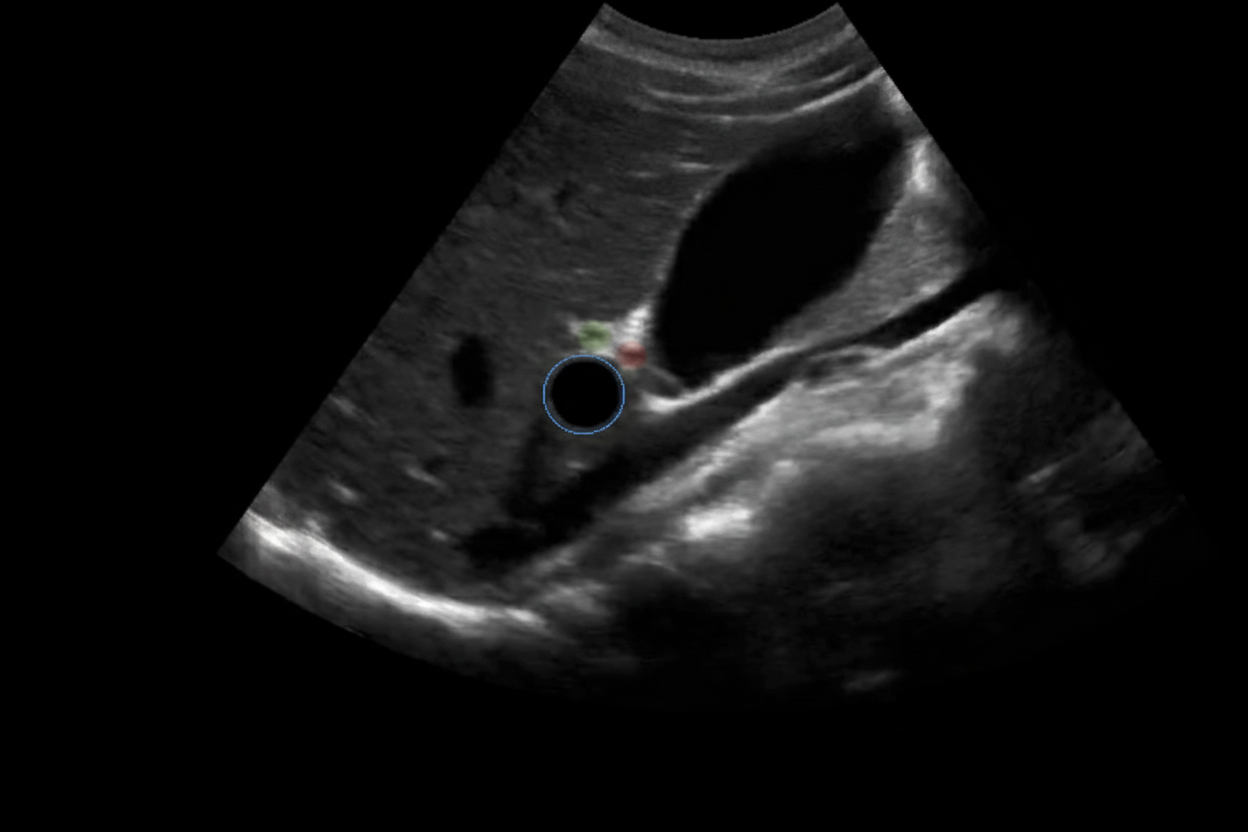
A 6-year-old baby is brought to the hospital by her parents complaining about right upper quadrant pain. On examination the baby is found to have jaundice and palpable abdominal mass. USG of the baby is shown below. What is the most likely cause?
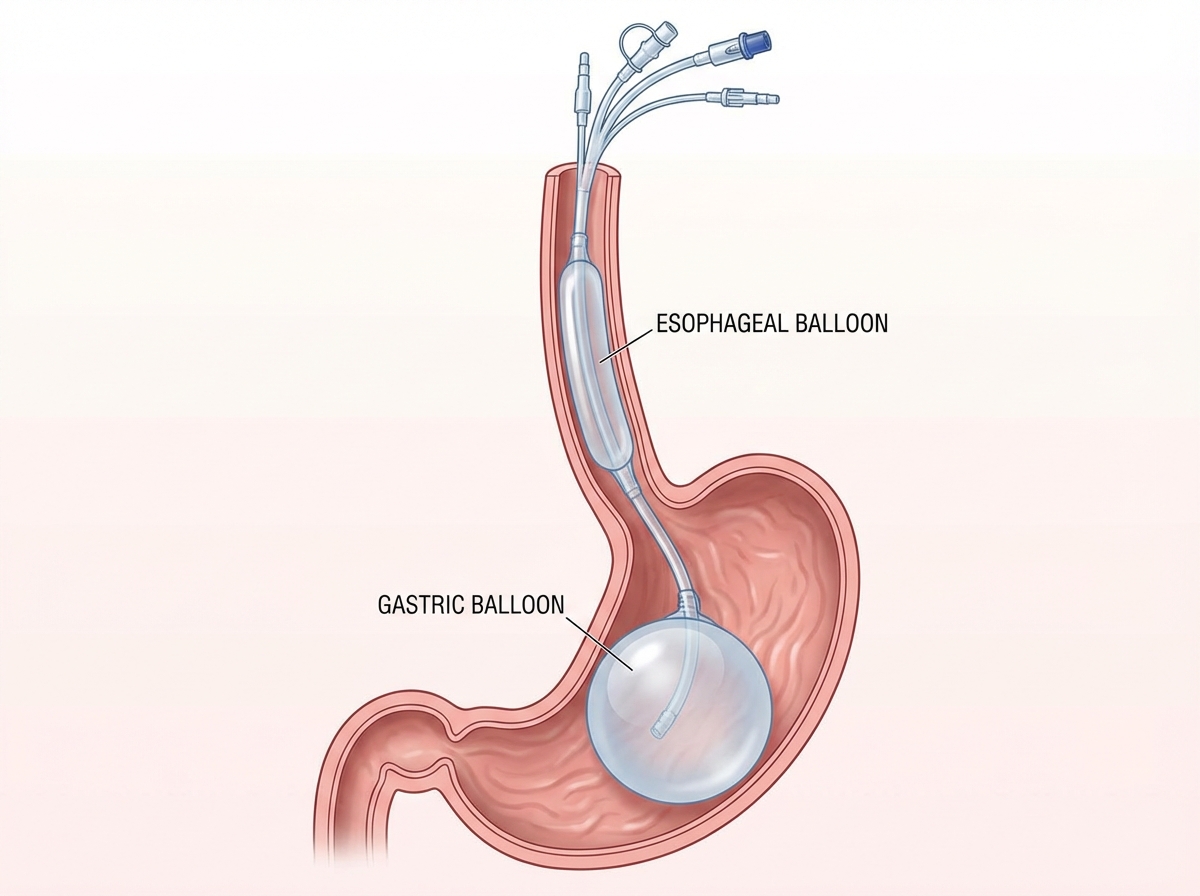
A 12-year-old patient with esophageal varices is managed by the procedure shown in the image. All of the following statements regarding this condition are true except:
What does the intraoperative image shown below depict?
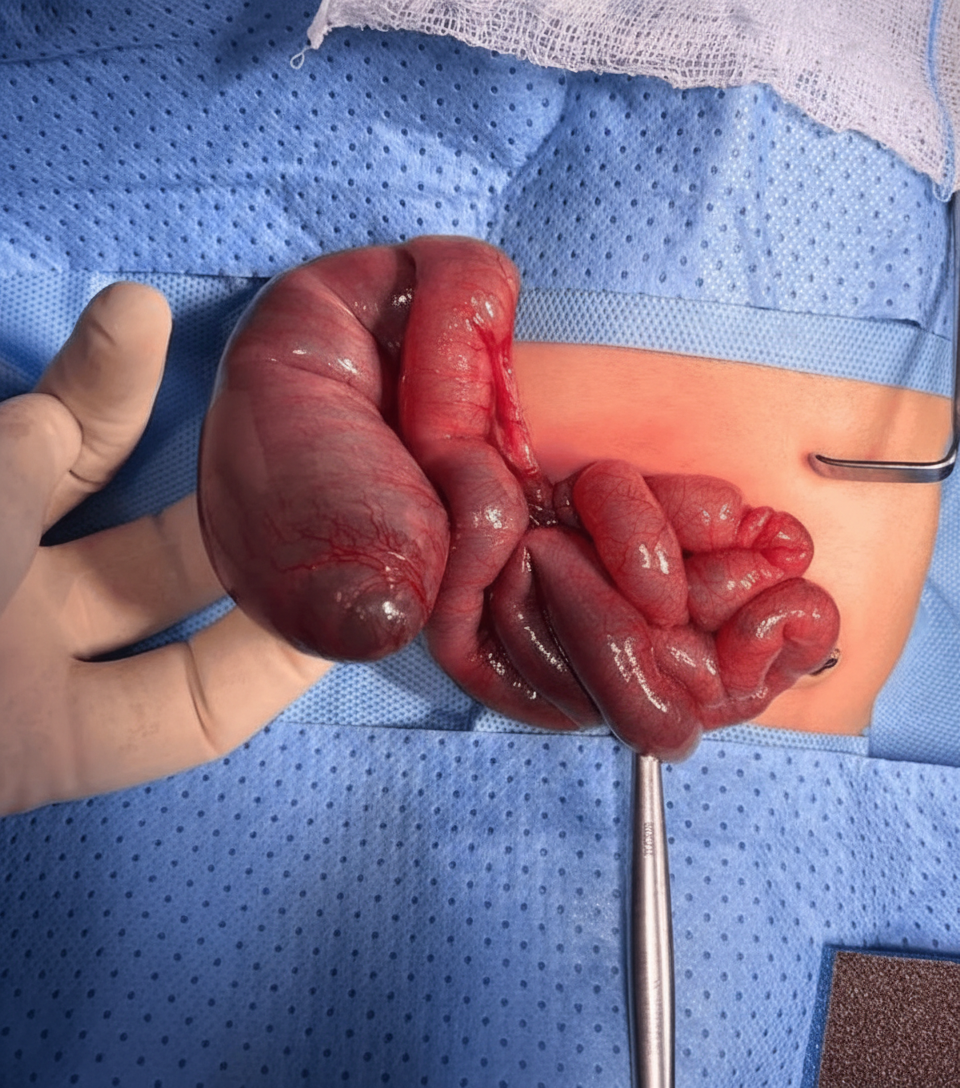
Which of the following is true regarding this condition?

Practice by Chapter
Biliary atresia and Kasai procedure
Practice Questions
Congenital abdominal wall defects
Practice Questions
Congenital diaphragmatic hernia
Practice Questions
Congenital heart defects requiring surgery
Practice Questions
Hirschsprung disease management
Practice Questions
Intussusception reduction techniques
Practice Questions
Necrotizing enterocolitis surgical management
Practice Questions
Neonatal surgical emergencies
Practice Questions
Pediatric fluid and electrolyte management
Practice Questions
Pediatric trauma considerations
Practice Questions
Pyloric stenosis diagnosis and pyloromyotomy
Practice Questions
Tracheoesophageal fistula repair
Practice Questions
Undescended testis and orchiopexy
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app