
Pediatric orthopedic emergencies — MCQs

A 6-week-old boy is brought for routine examination at his pediatrician’s office. The patient was born at 39 weeks to a 26-year-old G1P1 mother by normal vaginal delivery. External cephalic version was performed successfully at 37 weeks for breech presentation. Pregnancy was complicated by gestational diabetes that was well-controlled with insulin. The patient’s maternal grandmother has early onset osteoporosis. On physical examination, the left hip dislocates posteriorly with adduction and depression of a flexed femur. An ultrasound is obtained that reveals left acetabular dysplasia and a dislocated left femur. Which of the following is the next best step in management?
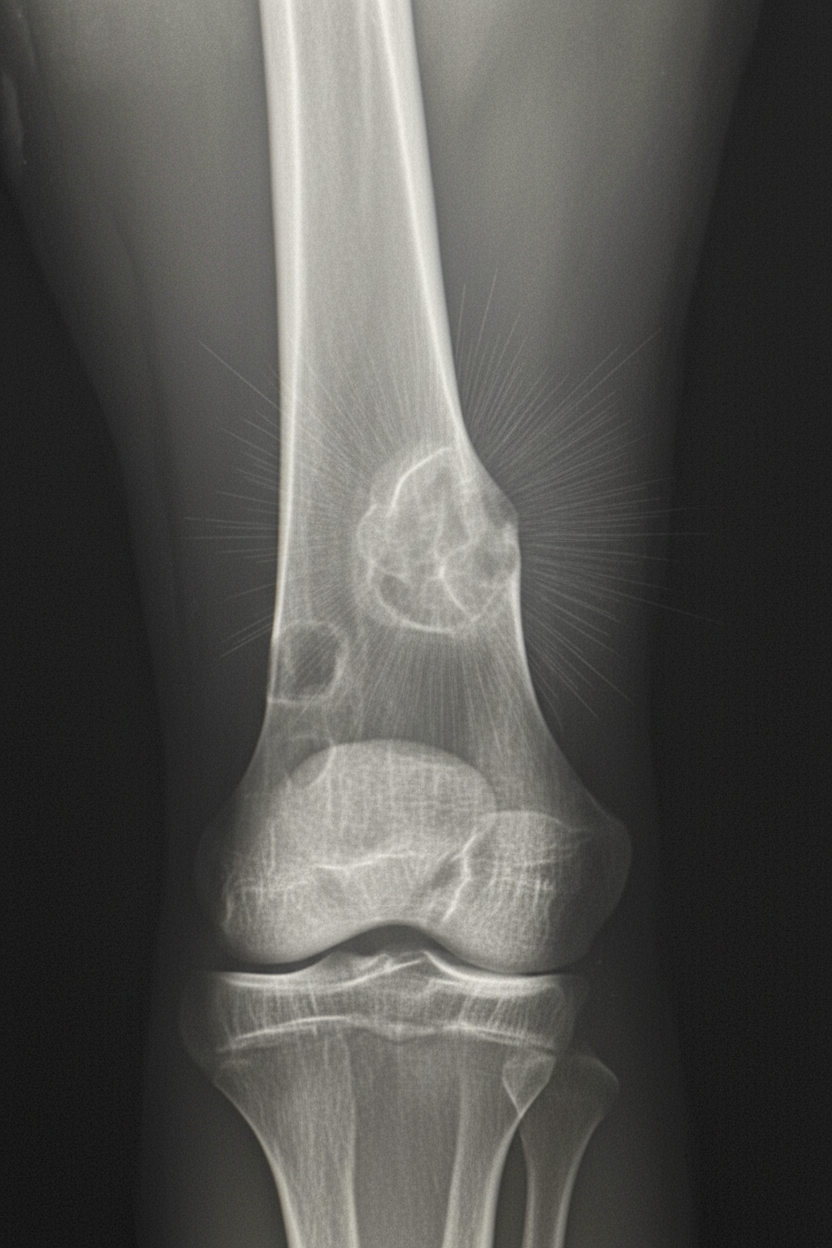
A 17-year-old boy is brought to the physician because of progressive right knee pain for the past 3 months. He reports that the pain is worse at night and while doing sports at school. He has not had any trauma to the knee or any previous problems with his joints. His vital signs are within normal limits. Examination of the right knee shows mild swelling and tenderness without warmth or erythema; the range of motion is limited. He walks with an antalgic gait. Laboratory studies show an alkaline phosphatase of 180 U/L and an erythrocyte sedimentation rate of 80 mm/h. An x-ray of the right knee is shown. Which of the following is the most likely diagnosis?
A 6-year-old boy is brought to the physician because of right hip pain that started that afternoon. His mother reports that he has also been limping since the pain developed. He says that the pain worsens when he moves or walks. He participated in a dance recital yesterday, but his mother believes that he was not injured at the time. He was born at term and has been healthy except for an episode of nasal congestion and mild cough 10 days ago. His mother has rheumatoid arthritis and his grandmother has osteoporosis. He is at the 50th percentile for height and 50th percentile for weight. His temperature is 37.5°C (99.6°F), pulse is 105/min, respirations are 16/min, and blood pressure is 90/78 mm Hg. His right hip is slightly abducted and externally rotated. Examination shows no tenderness, warmth, or erythema. He is able to bear weight. The remainder of the examination shows no abnormalities. Laboratory studies show a hemoglobin concentration of 12.3 g/dL, a leukocyte count of 8,500/mm3, and an erythrocyte sedimentation rate of 12 mm/h. Ultrasound of the right hip shows increased fluid within the joint. X-ray of the hips shows no abnormalities. Which of the following is the most likely diagnosis?
A 7-year-old boy is brought to the physician by his mother because of a limp for the last 3 weeks. He has also had right hip pain during this period. The pain is aggravated when he runs. He had a runny nose and fever around a month ago that resolved with over-the-counter medications. He has no history of serious illness. His development is adequate for his age. His immunizations are up-to-date. He appears healthy. He is at the 60th percentile for height and at 65th percentile for weight. Vital signs are within normal limits. Examination shows an antalgic gait. The right groin is tender to palpation. Internal rotation and abduction of the right hip is limited by pain. The remainder of the examination shows no abnormalities. His hemoglobin concentration is 11.6 g/dL, leukocyte count is 8,900/mm3, and platelet count is 130,000/mm3. An x-ray of the pelvis is shown. Which of the following is the most likely underlying mechanism?

A patient presents to the emergency department with arm pain. The patient recently experienced an open fracture of his radius when he fell from a ladder while cleaning his house. Surgical reduction took place and the patient's forearm was put in a cast. Since then, the patient has experienced worsening pain in his arm. The patient has a past medical history of hypertension and asthma. His current medications include albuterol, fluticasone, loratadine, and lisinopril. His temperature is 99.5°F (37.5°C), blood pressure is 150/95 mmHg, pulse is 90/min, respirations are 19/min, and oxygen saturation is 99% on room air. The patient's cast is removed. On physical exam, the patient's left arm is tender to palpation. Passive motion of the patient's wrist and fingers elicits severe pain. The patient's left radial and ulnar pulse are both palpable and regular. The forearm is soft and does not demonstrate any bruising but is tender to palpation. Which of the following is the next best step in management?
A 43-year-old man is brought to the emergency department 40 minutes after falling off a 10-foot ladder. He has severe pain and swelling of his right ankle and is unable to walk. He did not lose consciousness after the fall. He has no nausea. He appears uncomfortable. His temperature is 37°C (98.6°F), pulse is 98/min, respirations are 16/min, and blood pressure is 110/80 mm Hg. He is alert and oriented to person, place, and time. Examination shows multiple abrasions over both lower extremities. There is swelling and tenderness of the right ankle; range of motion is limited by pain. The remainder of the examination shows no abnormalities. An x-ray of the ankle shows an extra-articular calcaneal fracture. Intravenous analgesia is administered. Which of the following is the most appropriate next step in the management of this patient?
A 25-year-old man comes to the physician because of left-sided knee pain for 2 weeks. The pain started while playing basketball after suddenly hearing a popping sound. He has been unable to run since this incident. He has asthma, allergic rhinitis, and had a progressive bilateral sensorineural hearing impairment at birth treated with cochlear implants. His only medication is a salbutamol inhaler. The patient appears healthy and well-nourished. His temperature is 37°C (98.6°F), pulse is 67/min, and blood pressure is 120/80 mm Hg. Examination of the left knee shows medial joint line tenderness. Total knee extension is not possible and a clicking sound is heard when the knee is extended. An x-ray of the left knee shows no abnormalities. Which of the following is the most appropriate next step in the management of this patient?
A 17-year-old male presents to your office with right knee pain. He is the quarterback of his high school football team and developed the knee pain after being tackled in last night's game. He states he was running with the ball and was hit on the lateral aspect of his right knee while his right foot was planted. Now, he is tender to palpation over the medial knee and unable to bear full weight on the right lower extremity. A joint effusion is present and arthrocentesis yields 50 cc's of clear fluid. Which of the following exam maneuvers is most likely to demonstrate ligamentous laxity?
A 16-year-old man presents to the emergency department with a 2-hour history of sudden-onset abdominal pain. He was playing football when his symptoms started. The patient’s past medical history is notable only for asthma. Social history is notable for unprotected sex with 4 women in the past month. His temperature is 99.3°F (37.4°C), blood pressure is 120/88 mmHg, pulse is 117/min, respirations are 14/min, and oxygen saturation is 99% on room air. Physical exam is noted for a non-tender abdomen. Testicular exam reveals a right testicle which is elevated with a horizontal lie and the scrotum is neither swollen nor discolored. Which of the following is the most likely diagnosis?
A 31-year-old man presents to the Emergency Department with severe left leg pain and paresthesias 4 hours after his leg got trapped by the closing door of a bus. Initially, he had a mild pain which gradually increased to unbearable levels. Past medical history is noncontributory. In the Emergency Department, his blood pressure is 130/80 mm Hg, heart rate is 87/min, respiratory rate is 14/min, and temperature is 36.8℃ (98.2℉). On physical exam, his left calf is firm and severely tender on palpation. The patient cannot actively dorsiflex his left foot, and passive dorsiflexion is limited. Posterior tibial and dorsalis pedis pulses are 2+ in the right leg and 1+ in the left leg. Axial load does not increase the pain. Which of the following is the best next step in the management of this patient?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app