
Palliative surgical procedures — MCQs

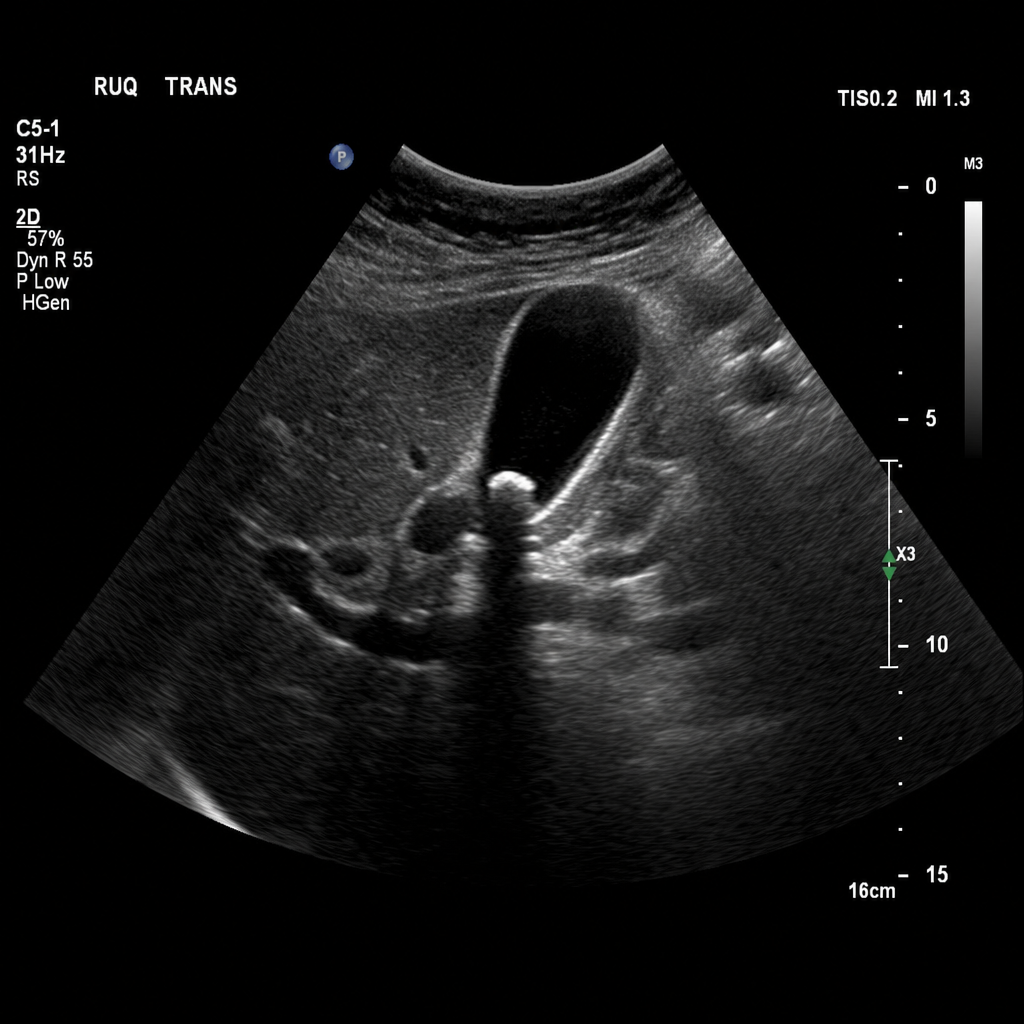
A 43-year-old Caucasian woman is admitted to the hospital with acute onset right upper quadrant (RUQ) pain. The pain started 6 hours ago after the patient had a large meal at a birthday party and has progressively worsened. She recalls having similar pain before but not so intense. No significant past medical history. Current medications are only oral contraceptive. Vitals are blood pressure 140/80 mm Hg, heart rate 79/min, respiratory rate 14/min, and temperature 37.6℃ (99.7℉). The patient’s BMI is 36.3 kg/m2. On exam, the patient appears slightly jaundiced. Her cardiac and respiratory examinations are within normal limits. Abdominal palpation reveals tenderness to palpation in the RUQ with no rebound or guarding, and there is an inspiratory arrest on deep palpation in this region. The remainder of the examination is within normal limits. Laboratory tests are significant for the following: RBC count 4.1 million/mm3 Hb 13.4 mg/dL Leukocyte count 11,200/mm3 ESR 22 mm/hr Platelet count 230,000/mm3 Total bilirubin 2 mg/dL Direct bilirubin 1.1 mg/dL ALT 20 IU/L AST 18 IU/L Amylase 33 IU/L Ultrasound of the abdomen shows the following result (see image): The common bile duct (CBD) (not shown in the image) is not dilated. Which of the following procedures is most appropriate for the treatment of this patient?
A 53-year-old woman comes to the emergency department because of weakness and abdominal pain for 24 hours. She has had three bowel movements with dark stool during this period. She has not had vomiting and has never had such episodes in the past. She underwent a tubal ligation 15 years ago. She has chronic lower extremity lymphedema, osteoarthritis, and type 2 diabetes mellitus. Her father died of colon cancer at the age of 72 years. Current medications include metformin, naproxen, and calcium with vitamin D3. She had a screening colonoscopy at 50 years of age which was normal. She appears pale and diaphoretic. Her temperature is 36°C (96.8°F), pulse is 110/min, respirations are 20/min, and blood pressure is 90/50 mm Hg. Pulse oximetry on room air shows an oxygen saturation of 98%. The abdomen is soft and nondistended with mild epigastric tenderness. Rectal exam shows tarry stool. Two large bore IV lines are placed and fluid resuscitation with normal saline is initiated. Which of the following is the most appropriate next step in management?
A 19-year-old woman is diagnosed with metastatic Ewing sarcoma. She has undergone multiple treatments without improvement. She decides to stop treatment and pursue only palliative care. She is of sound mind and has weighed the benefits and risks of this decision. The patient’s mother objects and insists that treatments be continued. What should be done?
A 62-year-old woman presents to her oncologist to discuss the chemotherapy options for her newly diagnosed breast cancer. During the meeting, they discuss a drug that inhibits the breakdown of mitotic spindles in cells. Her oncologist explains that this will be more toxic to cancer cells because those cells are dividing more rapidly. Which of the following side effects is closely associated with the use of this chemotherapeutic agent?
One week after admission to the hospital for an extensive left middle cerebral artery stroke, a 91-year-old woman is unable to communicate, walk, or safely swallow food. She has been without nutrition for the duration of her hospitalization. The patient's sister requests placement of a percutaneous endoscopic gastrostomy tube for nutrition. The patient's husband declines the intervention. There is no living will. Which of the following is the most appropriate course of action by the physician?
A previously healthy 37-year-old man comes to the physician for the evaluation of an 8-week history of intermittent burning epigastric pain. During this period, he has also felt bloated and uncomfortable after meals. He has not had weight loss or a change in bowel habits. He has no personal or family history of serious illness. He takes no medications. He does not smoke. He drinks 1–3 beers per week. Vital signs are within normal limits. Abdominal examination shows mild epigastric tenderness on palpation without guarding or rebound tenderness. Bowel sounds are normal. The remainder of the examination shows no abnormalities. Which of the following is the most appropriate next step in management?
A 68-year-old man comes to the emergency department because of sudden onset abdominal pain for 6 hours. On a 10-point scale, he rates the pain as a 8 to 9. The abdominal pain is worst in the right upper quadrant. He has atrial fibrillation and hyperlipidemia. His temperature is 38.7° C (101.7°F), pulse is 110/min, and blood pressure is 146/86 mm Hg. The patient appears acutely ill. Physical examination shows a distended abdomen and tenderness to palpation in all quadrants with guarding, but no rebound. Murphy's sign is positive. Right upper quadrant ultrasound shows thickening of the gallbladder wall, sludging in the gallbladder, and pericolic fat stranding. He is admitted for acute cholecystitis and grants permission for cholecystectomy. His wife is his healthcare power of attorney (POA), but she is out of town on a business trip. He is accompanied today by his brother. After induction and anesthesia, the surgeon removes the gallbladder but also finds a portion of the small intestine is necrotic due to a large thromboembolism occluding a branch of the superior mesenteric artery. The treatment is additional surgery with small bowel resection and thromboendarterectomy. Which of the following is the most appropriate next step in management?
A terminally ill patient with advanced cancer requests that no resuscitation be performed in the event of cardiac arrest. The patient is mentally competent and has completed advance directives. A family member later demands full resuscitation efforts. Which of the following is the most appropriate response?
A 66-year-old man comes to the physician because of yellowish discoloration of his eyes and skin, abdominal discomfort, and generalized fatigue for the past 2 weeks. He has had dark urine and pale stools during this period. He has had a 10-kg (22-lb) weight loss since his last visit 6 months ago. He has hypertension. He has smoked one pack of cigarettes daily for 34 years. He drinks three to four beers over the weekends. His only medication is amlodipine. His temperature is 37.3°C (99.1°F), pulse is 89/min, respirations are 14/min, and blood pressure is 114/74 mm Hg. Examination shows jaundice of the sclera and skin and excoriation marks on his trunk and extremities. The lungs are clear to auscultation. The abdomen is soft and nontender. The remainder of the examination shows no abnormalities. Laboratory studies show: Hemoglobin 12 g/dL Leukocyte count 5,000/mm3 Platelet count 400,000/mm3 Serum Urea nitrogen 28 mg/dL Creatinine 1.2 mg/dL Bilirubin Total 7.0 mg/dL Direct 5.5 mg/dL Alkaline phosphatase 615 U/L Aspartate aminotransferase (AST, GOT) 170 U/L Alanine aminotransferase (ALT, GPT) 310 U/L γ-Glutamyltransferase (GGT) 592 U/L (N = 5–50 U/L) An ultrasound shows extrahepatic biliary dilation. A CT scan of the abdomen shows a 2.5-cm (1-in) mass in the head of the pancreas with no abdominal lymphadenopathy. The patient undergoes biliary stenting. Which of the following is the most appropriate next step in the management of this patient?
A 63-year-old female with known breast cancer presents with progressive motor weakness in bilateral lower extremities and difficulty ambulating. Physical exam shows 4 of 5 motor strength in her legs and hyper-reflexia in her patellar tendons. Neurologic examination 2 weeks prior was normal. Imaging studies, including an MRI, show significant spinal cord compression by the metastatic lesion and complete erosion of the T12 vertebrae. She has no metastatic disease to the visceral organs and her oncologist reports her life expectancy to be greater than one year. What is the most appropriate treatment?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app