
Cytoreductive surgery principles — MCQs

The surgical equipment used during a craniectomy is sterilized using pressurized steam at 121°C for 15 minutes. Reuse of these instruments can cause transmission of which of the following pathogens?
A 19-year-old woman presents to her gynecologist for evaluation of amenorrhea and occasional dull right-sided lower abdominal pain that radiates to the rectum. She had menarche at 11 years of age and had regular 28-day cycles by 13 years of age. She developed menstrual cycle irregularity approximately 2 years ago and has not had a menses for 6 months. She is not sexually active. She does not take any medications. Her weight is 94 kg (207.2 lb) and her height is 166 cm (5.4 ft). Her vital signs are within normal limits. The physical examination shows a normal hair growth pattern. No hair loss or acne are noted. There is black discoloration of the skin in the axillae and posterior neck. Palpation of the abdomen reveals slight tenderness in the right lower quadrant, but no masses are appreciated. The gynecologic examination reveals no abnormalities. The hymen is intact. The rectal examination reveals a non-tender, mobile, right-sided adnexal mass. Which of the following management plans would be best for this patient?
A 57-year-old female presents to general gynecology clinic for evaluation of a pelvic mass. The mass was detected on a routine visit to her primary care doctor during abdominal palpation. In the office, she receives a transvaginal ultrasound, which reveals a mass measuring 11 cm in diameter. In the evaluation of this mass, elevation of which tumor marker would be suggestive of an ovarian cancer?
One day after undergoing an open colectomy, a 65-year-old man with colon cancer experiences shivers. The procedure was originally scheduled to be done laparoscopically, but it was converted because of persistent bleeding. Besides the conversion, the operation was uneventful. Five years ago, he underwent renal transplantation because of cystic disease and has been taking prednisolone since then. He has a history of allergy to sulfonamides. He appears acutely ill. His temperature is 39.2°C (102.5°F), pulse is 120/min, respirations are 23/min, and blood pressure is 90/62 mm Hg. Abdominal examination shows a midline incision extending from the xiphisternum to the pubic symphysis. There is a 5-cm (2-in) area of purplish discoloration near the margin of the incision in the lower abdomen. Palpation of the abdomen produces severe pain and crackling sounds are heard. Laboratory studies show: Hemoglobin 12.5 g/dL Leukocyte count 18,600/mm3 Platelet count 228,000/mm3 Erythrocyte sedimentation rate 120 mm/h Serum Na+ 134 mEq/L K+ 3.5 mEq/L Cl- 98 mEq/L HCO3- 22 mEq/L Glucose 200 mg/dL Urea nitrogen 60 mg/dL Creatinine 3.2 mg/dL Creatine kinase 750 U/L Which of the following is the most appropriate next step in management?
A 32-year-old man is brought to the emergency department after a skiing accident. The patient had been skiing down the mountain when he collided with another skier who had stopped suddenly in front of him. He is alert but complaining of pain in his chest and abdomen. He has a past medical history of intravenous drug use and peptic ulcer disease. He is a current smoker. His temperature is 97.4°F (36.3°C), blood pressure is 77/53 mmHg, pulse is 127/min, and respirations are 13/min. He has a GCS of 15 and bilateral shallow breath sounds. His abdomen is soft and distended with bruising over the epigastrium. He is moving all four extremities and has scattered lacerations on his face. His skin is cool and delayed capillary refill is present. Two large-bore IVs are placed in his antecubital fossa, and he is given 2L of normal saline. His FAST exam reveals fluid in Morison's pouch. Following the 2L normal saline, his temperature is 97.5°F (36.4°C), blood pressure is 97/62 mmHg, pulse is 115/min, and respirations are 12/min. Which of the following is the best next step in management?
A 56-year-old woman is one week status post abdominal hysterectomy when she develops a fever of 101.4°F (38.6°C). Her past medical history is significant for type II diabetes mellitus and a prior history of alcohol abuse. The operative report and intraoperative cystoscopy indicate that the surgery was uncomplicated. The nurse reports that since the surgery, the patient has also complained of worsening lower abdominal pain. She has given the patient the appropriate pain medications with little improvement. The patient has tolerated an oral diet well and denies nausea, vomiting, or abdominal distension. Her blood pressure is 110/62 mmHg, pulse is 122/min, and respirations are 14/min. Since being given 1000 mL of intravenous fluids yesterday, the patient has excreted 800 mL of urine. On physical exam, she is uncomfortable, shivering, and sweating. The surgical site is intact, but the surrounding skin appears red. No drainage is appreciated. The abdominal examination reveals tenderness to palpation and hypoactive bowel sounds. Labs and a clean catch urine specimen are obtained as shown below: Leukocyte count and differential: Leukocyte count: 18,000/mm^3 Segmented neutrophils: 80% Bands: 10% Eosinophils: 1% Basophils: < 1% Lymphocytes: 5% Monocytes: 4% Platelet count: 300,000/mm^3 Hemoglobin: 12.5 g/dL Hematocrit: 42% Urine: Epithelial cells: 15/hpf Glucose: positive RBC: 1/hpf WBC: 2/hpf Bacteria: 50 cfu/mL Ketones: none Nitrites: negative Leukocyte esterase: negative Which of the following is most likely the cause of this patient’s symptoms?
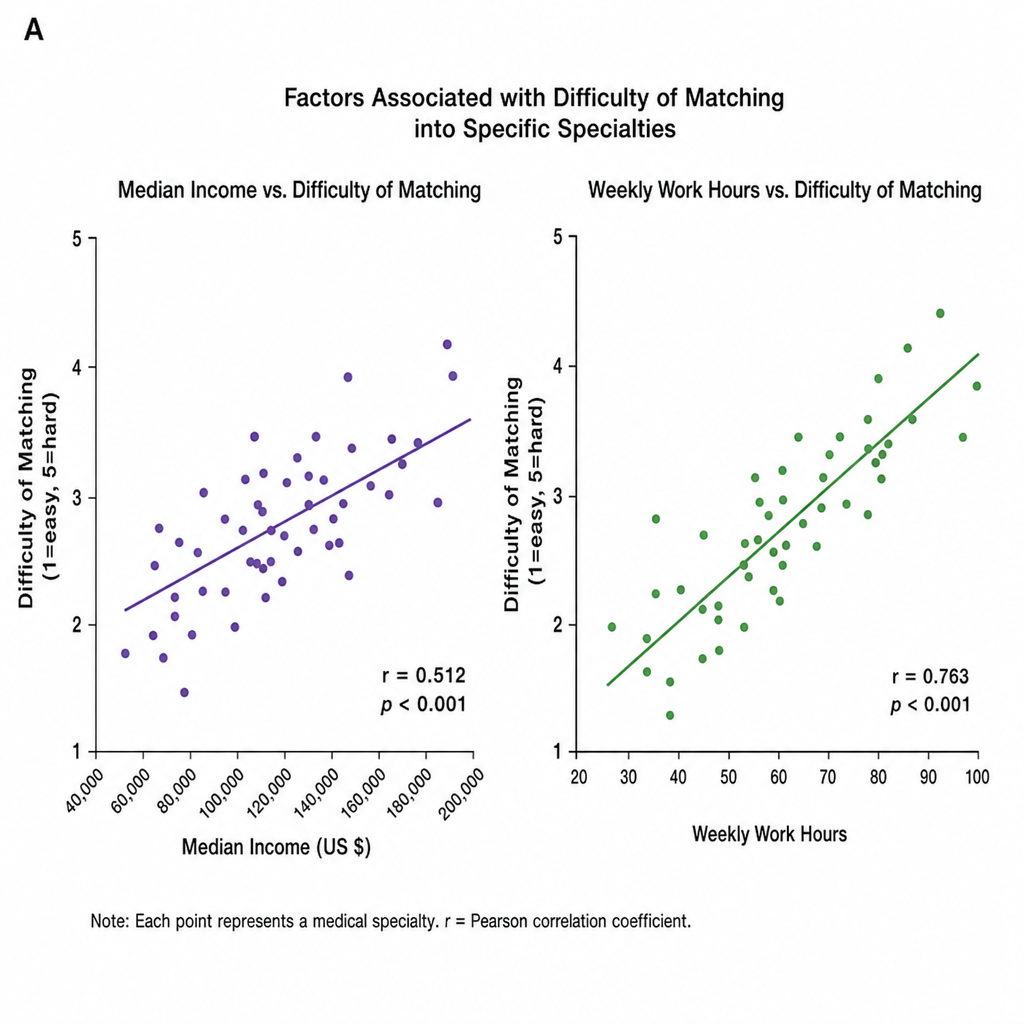
Confident of your performance on Step 1 given your extensive utilization of Medbullets, you preemptively start to ponder your future specialty choice. You come across an analysis of lifestyle factors and how they affect medical student specialty choices. Image A depicts two scatter plots comparing the relationship between median income and weekly work hours on the difficulty of matching into specific specialties. Both associations are statistically significant. Which statement best describes the results?
A 28-year-old male presents to his primary care physician with complaints of intermittent abdominal pain and alternating bouts of constipation and diarrhea. His medical chart is not significant for any past medical problems or prior surgeries. He is not prescribed any current medications. Which of the following questions would be the most useful next question in eliciting further history from this patient?
A 65-year-old man is admitted to the hospital because of a 1-month history of fatigue, intermittent fever, and weakness. Results from a peripheral blood smear taken during his evaluation are indicative of possible acute myeloid leukemia. Bone marrow aspiration and subsequent cytogenetic studies confirm the diagnosis. The physician sets aside an appointed time-slot and arranges a meeting in a quiet office to inform him about the diagnosis and discuss his options. He has been encouraged to bring someone along to the appointment if he wanted. He comes to your office at the appointed time with his daughter. He appears relaxed, with a full range of affect. Which of the following is the most appropriate opening statement in this situation?
A previously healthy 25-year-old woman is brought to the emergency department because of a 1-hour history of sudden severe lower abdominal pain. The pain started shortly after having sexual intercourse. The pain is worse with movement and urination. The patient had several urinary tract infections as a child. She is sexually active with her boyfriend and uses condoms inconsistently. She cannot remember when her last menstrual period was. She appears uncomfortable and pale. Her temperature is 37.5°C (99.5°F), pulse is 110/min, and blood pressure is 90/60 mm Hg. Abdominal examination shows a palpable, tender right adnexal mass. Her hemoglobin concentration is 10 g/dL and her hematocrit is 30%. A urine pregnancy test is negative. Pelvic ultrasound shows a 5 x 3-cm right ovarian sac-like structure with surrounding echogenic fluid around the structure and the uterus. Which of the following is the most appropriate management for this patient's condition?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app