
Subdural and epidural hematoma management — MCQs

A previously healthy 10-year-old boy is brought to the emergency department for the evaluation of one episode of vomiting and severe headache since this morning. His mother says he also had difficulty getting dressed on his own. He has not had any trauma. The patient appears nervous. His temperature is 37°C (98.6°F), pulse is 100/min, and blood pressure is 185/125 mm Hg. He is confused and oriented only to person. Ophthalmic examination shows bilateral optic disc swelling. There is an abdominal bruit that is best heard at the right costovertebral angle. A complete blood count is within normal limits. Which of the following is most likely to confirm the diagnosis?
A 68-year-old man is brought to the emergency department because of a severe headache, nausea, and vomiting for 30 minutes. Forty-five minutes ago, he fell and struck his head, resulting in loss of consciousness for 1 minute. After regaining consciousness, he felt well for 15 minutes before the headache began. On arrival, the patient becomes rigid and his eyes deviate to the right; he is incontinent of urine. Intravenous lorazepam is administered and the rigidity resolves. Which of the following is the most likely cause of the patient's condition?
A 15-year-old boy is brought to the emergency department one hour after sustaining an injury during football practice. He collided head-on into another player while wearing a mouthguard and helmet. Immediately after the collision he was confused but able to use appropriate words. He opened his eyes spontaneously and followed commands. There was no loss of consciousness. He also had a headache with dizziness and nausea. He is no longer confused upon arrival. He feels well. Vital signs are within normal limits. He is fully alert and oriented. His speech is organized and he is able to perform tasks demonstrating full attention, memory, and balance. Neurological examination shows no abnormalities. There is mild tenderness to palpation over the crown of his head but no signs of skin break or fracture. Which of the following is the most appropriate next step?
A 60-year-old male is admitted to the ICU for severe hypertension complicated by a headache. The patient has a past medical history of insulin-controlled diabetes, hypertension, and hyperlipidemia. He smokes 2 packs of cigarettes per day. He states that he forgot to take his medications yesterday and started getting a headache about one hour ago. His vitals on admission are the following: blood pressure of 160/110 mmHg, pulse 95/min, temperature 98.6 deg F (37.2 deg C), and respirations 20/min. On exam, the patient has an audible abdominal bruit. After administration of antihypertensive medications, the patient has a blood pressure of 178/120 mmHg. The patient reports his headache has increased to a 10/10 pain level, that he has trouble seeing, and he can't move his extremities. After stabilizing the patient, what is the best next step to diagnose the patient's condition?
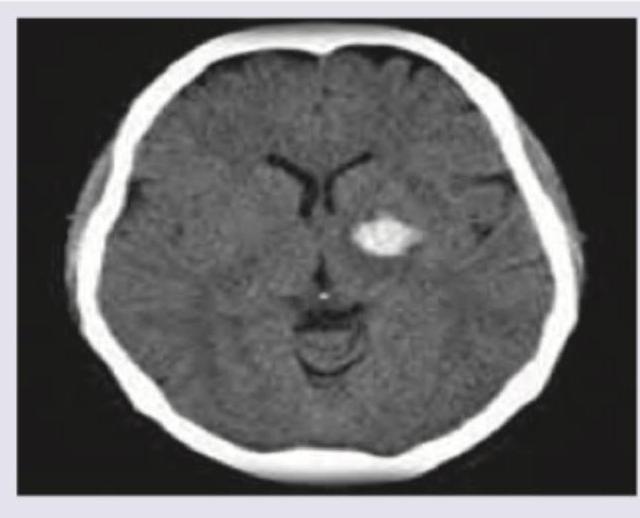
A 53-year-old man is brought to the emergency department for confusion. He was in his usual state of health until about 3 hours ago when he tried to use his sandwich to turn off the TV. He also complained to his wife that he had a severe headache. Past medical history is notable for hypertension, which has been difficult to control on multiple medications. His temperature is 36.7°C (98°F), the pulse is 70/min, and the blood pressure is 206/132 mm Hg. On physical exam he is alert and oriented only to himself, repeating over and over that his head hurts. The physical exam is otherwise unremarkable and his neurologic exam is nonfocal. The noncontrast CT scan of the patient's head is shown and reveals an acute intraparenchymal hemorrhage in the basal ganglia. Which of the following diagnostic tests would be most helpful in determining the underlying cause of this patient's hemorrhage?
A 2-month-old boy is brought to the emergency room by his mother who reports he has appeared lethargic for the past 3 hours. She reports that she left the patient with a new nanny this morning, and he was behaving normally. When she got home in the afternoon, the patient seemed lethargic and would not breastfeed as usual. At birth, the child had an Apgar score of 8/9 and weighed 2.8 kg (6.1 lb). Growth has been in the 90th percentile, and the patient has been meeting all developmental milestones. There is no significant past medical history, and vaccinations are up-to-date. On physical examination, the patient does not seem arousable. Ophthalmologic examination shows retinal hemorrhages. Which of the following findings would most likely be expected on a noncontrast CT scan of the head?
A 52-year-old woman is accompanied by her husband to the emergency department with a severe occipital headache that started suddenly an hour ago. She is drowsy but able to answer the physician's questions. She describes it as the worst headache she has ever had, 9/10 in intensity. The husband says it was initially localized to the occiput but has now spread all over her head and she also complained of a generalized heaviness. She took an ibuprofen without experiencing any relief. She also complains of blurry vision and nausea and had 1 episode of vomiting. She denies a recent history of fever, chills, numbness, or seizures. Her past medical history is significant for hypertension controlled with lisinopril and metoprolol. On examination, she is drowsy but oriented. Papilledema is seen on ophthalmoscopy. Neck flexion is difficult and painful. The rest of the exam is unremarkable. Her blood pressure is 160/100 mm Hg, heart rate is 100/min, and temperature is 37.0°C (98.6°F). The ECG, cardiac enzymes, and laboratory studies are normal. Lumbar puncture results are as follows: Opening pressure 210 mm H2O RBC 50/mm3, numbers steady over 4 test tubes Cell count 5/mm3 Glucose 60 mg/dL Proteins 100 mg/dL The patient is admitted to the ICU for further management. Which of the following is the most likely pathophysiology based on her history and CSF findings?
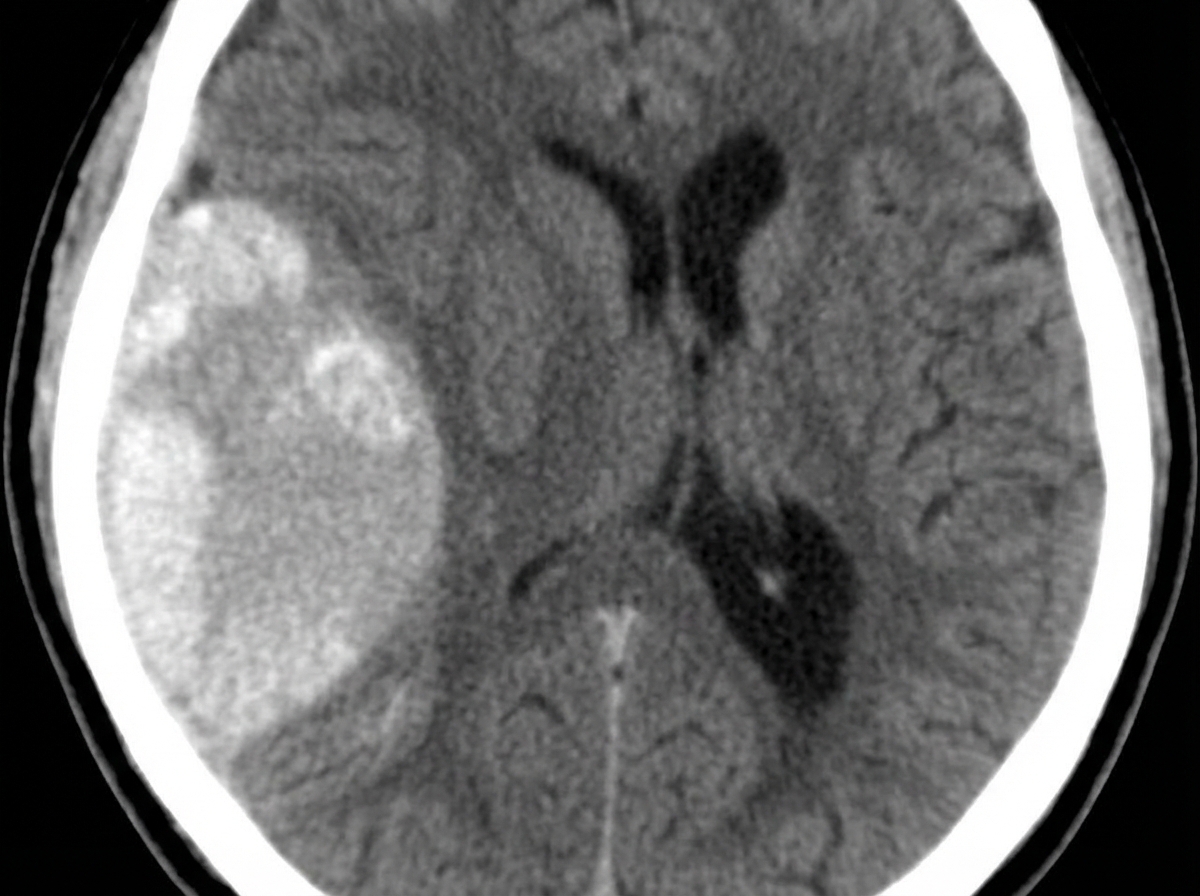
A 23-year-old man presents with a blunt force injury to the head from a baseball bat. He is currently unconscious, although his friends say he was awake and speaking with them en route to the hospital. He has no significant past medical history and takes no current medications. The vital signs include: temperature 37.0°C (98.6°F), blood pressure 165/85 mm Hg, pulse 50/min, and respiratory rate 19/min. On physical examination, there is a blunt force injury to the left temporoparietal region approximately 10.1–12.7 cm (4–5 in) in diameter. There is anisocoria of the left pupil, which is unresponsive to light. The patient is intubated and fluid resuscitation is initiated. A noncontrast computed tomography (CT) scan of the head is acquired and shown in the exhibit (see image). Which of the following is the most appropriate medical treatment for this patient?
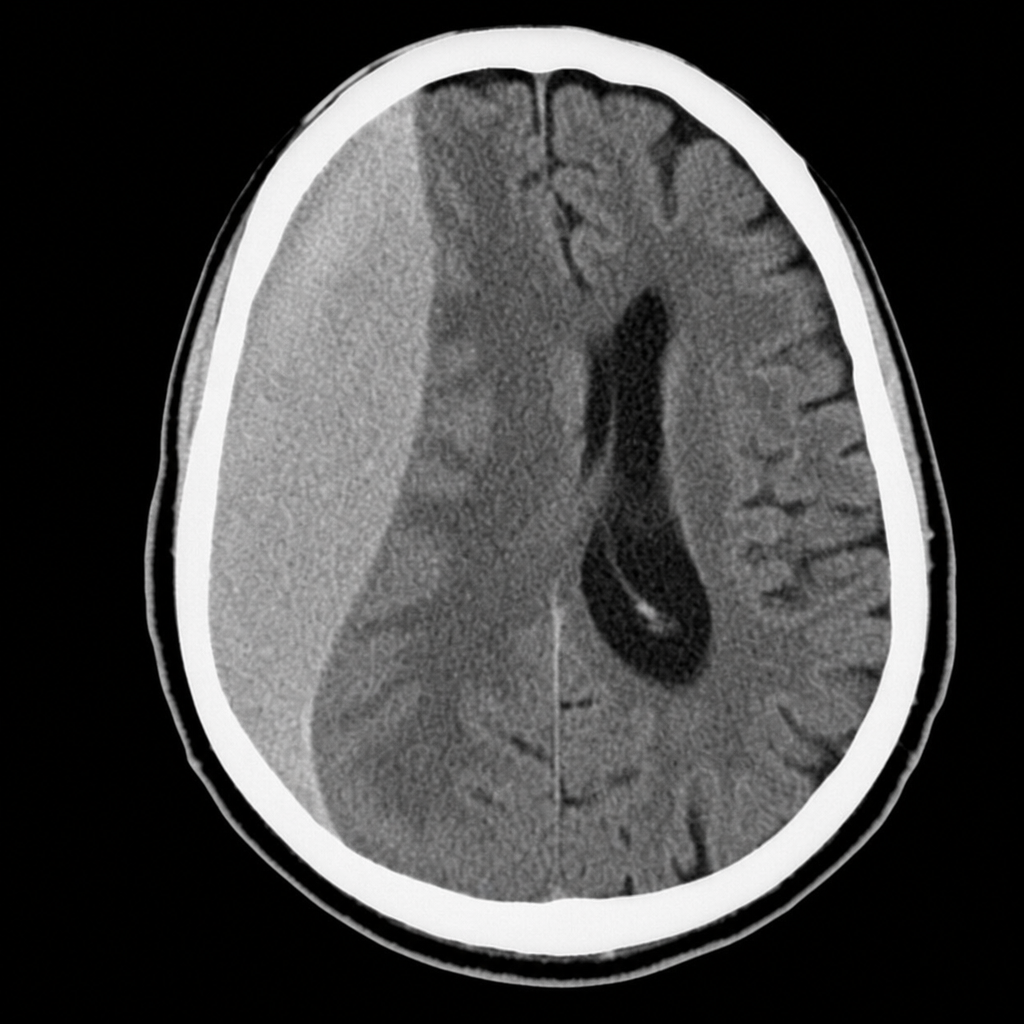
A 68-year-old man is brought to the clinic by his daughter who has noticed behavioral changes and frequent headaches for the past 2 weeks. The patient’s daughter says he has been having memory and simple calculation issues, gets upset easily, and his grip strength has dramatically declined. The patient was completely normal prior to these recent changes and used to be able to perform his activities of daily living without a problem. He has a past medical history significant for hypertension, stable angina, and benign prostatic hypertrophy, as well as frequent falls with the last one occurring 1 month ago. Physical examination is remarkable for dyscalculia, short-term memory deficits, and decreased grip strength (4/5) in his right hand. A noncontrast CT of the head is performed and is shown in the image. Which of the following is the most likely etiology of this patient condition?
A 77-year-old man is brought to the emergency department by his wife because of headache, nausea, and vomiting for 24 hours. His wife says that over the past 2 weeks, he has been more irritable and has had trouble remembering to do routine errands. Two weeks ago, he fell during a skiing accident but did not lose consciousness. He has coronary artery disease and hypertension. He has smoked one pack of cigarettes daily for 50 years. He has had 2 glasses of wine daily since his retirement 10 years ago. Current medications include atenolol, enalapril, furosemide, atorvastatin, and aspirin. He appears acutely ill. He is oriented to person but not to place or time. His temperature is 37°C (98.6°F), pulse is 99/min, respirations are 16/min, and blood pressure is 160/90 mm Hg. During the examination, he is uncooperative and unable to answer questions. Deep tendon reflexes are 4+ on the left and 2+ on the right. Babinski's sign is present on the left. There is mild weakness of the left iliopsoas and hamstring muscles. A CT scan of the head without contrast shows a high-density, 15-mm crescentic collection across the right hemispheric convexity. Which of the following is the most appropriate next step in the management of this patient?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app