
Cerebral aneurysm management — MCQs

A 21-year-old man presents to the emergency department after sustaining a stab wound to the neck at a local farmer's market. The patient is otherwise healthy and is complaining of pain. The patient is able to offer the history himself. His temperature is 97.6°F (36.4°C), blood pressure is 120/84 mmHg, pulse is 90/min, respirations are 15/min, and oxygen saturation is 98% on room air. Physical exam demonstrates a 3 cm laceration 1 cm inferior to the mastoid process on the right side. The patient's breath sounds are clear and he is protecting his airway. No stridor or difficulty breathing is noted. Which of the following is the most appropriate next step in the management of this patient?
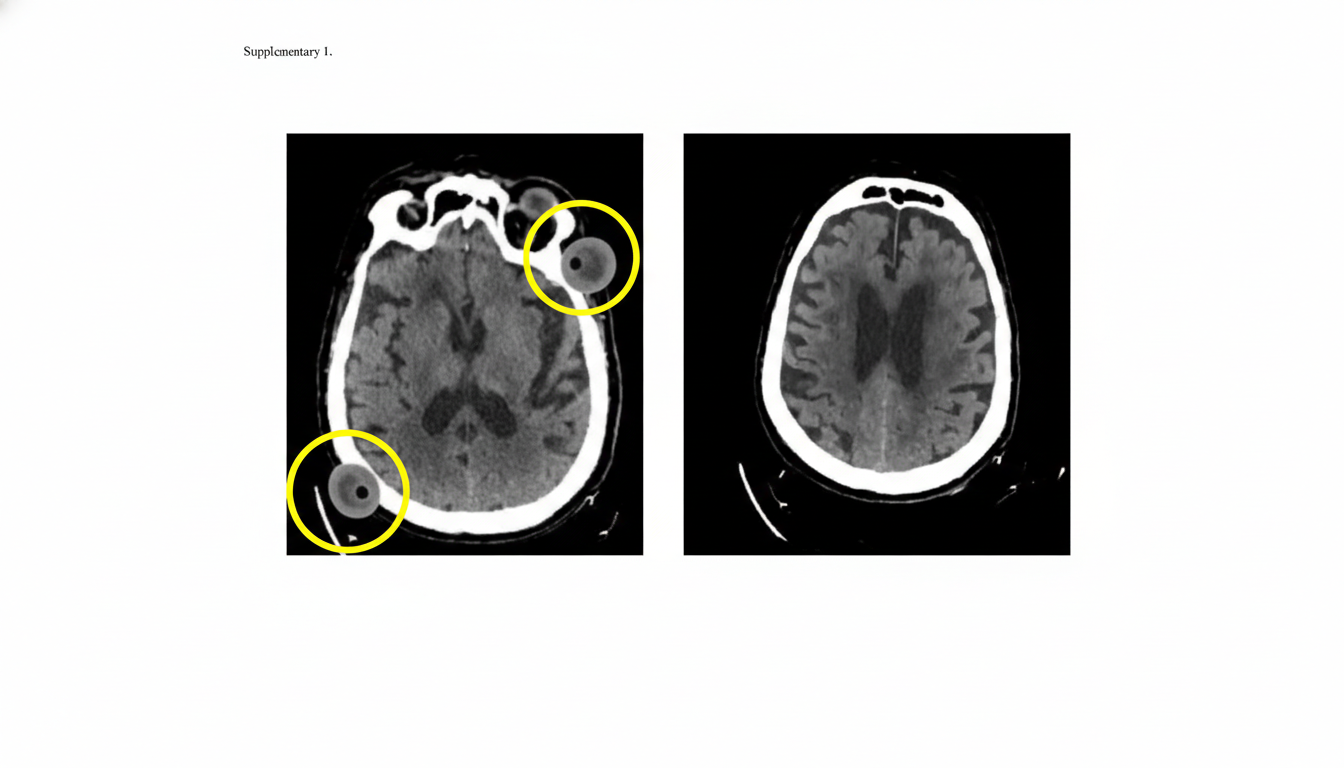
A 60-year-old man is brought to the emergency department by his wife with a sudden onset of right-sided weakness 2 hours ago. He can speak clearly without difficulty and denies any similar symptoms in the past. Past medical history is significant for hypertension and diabetes, both poorly managed due to medication non-compliance. Family history is significant for heart disease and diabetes in multiple paternal and maternal relatives. His vital signs include: blood pressure 150/88 mm Hg, pulse 86/min, and respiratory rate 15/min. On physical examination, strength is 3/5 on the right and 5/5 on the left upper and lower extremities. The sensation is intact, and no impairments in balance or ataxias are present. An initial noncontrast CT scan of the head is unremarkable, but a repeat noncontrast CT scan of the head performed a month later reveals the 2 lesions circled in the image. Which of the following is the most likely diagnosis in this patient?
A 52-year-old woman is brought to the emergency department for a severe, sudden-onset headache, light-sensitivity, and neck stiffness that began 30 minutes ago. A CT scan of the head shows hyperdensity between the arachnoid mater and the pia mater. The patient undergoes an endovascular procedure. One week later, she falls as she is returning from the bathroom. Neurologic examination shows 3/5 strength in the right lower extremity and 5/5 in the left lower extremity. Treatment with which of the following drugs is most likely to have prevented the patient's current condition?
A 60-year-old male is admitted to the ICU for severe hypertension complicated by a headache. The patient has a past medical history of insulin-controlled diabetes, hypertension, and hyperlipidemia. He smokes 2 packs of cigarettes per day. He states that he forgot to take his medications yesterday and started getting a headache about one hour ago. His vitals on admission are the following: blood pressure of 160/110 mmHg, pulse 95/min, temperature 98.6 deg F (37.2 deg C), and respirations 20/min. On exam, the patient has an audible abdominal bruit. After administration of antihypertensive medications, the patient has a blood pressure of 178/120 mmHg. The patient reports his headache has increased to a 10/10 pain level, that he has trouble seeing, and he can't move his extremities. After stabilizing the patient, what is the best next step to diagnose the patient's condition?
A 69-year-old male presents to the emergency department for slurred speech and an inability to use his right arm which occurred while he was eating dinner. The patient arrived at the emergency department within one hour. A CT scan was performed of the head and did not reveal any signs of hemorrhage. The patient is given thrombolytics and is then managed on the neurology floor. Three days later, the patient is recovering and is stable. He seems depressed but is doing well with his symptoms gradually improving as compared to his initial presentation. The patient complains of neck pain that has worsened slowly over the past few days for which he is being given ibuprofen. Laboratory values are ordered and return as indicated below: Serum: Na+: 130 mEq/L K+: 3.7 mEq/L Cl-: 100 mEq/L HCO3-: 24 mEq/L Urea nitrogen: 7 mg/dL Glucose: 70 mg/dL Creatinine: 0.9 mg/dL Ca2+: 9.7 mg/dL Urine: Appearance: dark Glucose: negative WBC: 0/hpf Bacterial: none Na+: 320 mEq/L/24 hours His temperature is 99.5°F (37.5°C), pulse is 95/min, blood pressure is 129/70 mmHg, respirations are 10/min, and oxygen saturation is 98% on room air. Which of the following is the best next step in management?
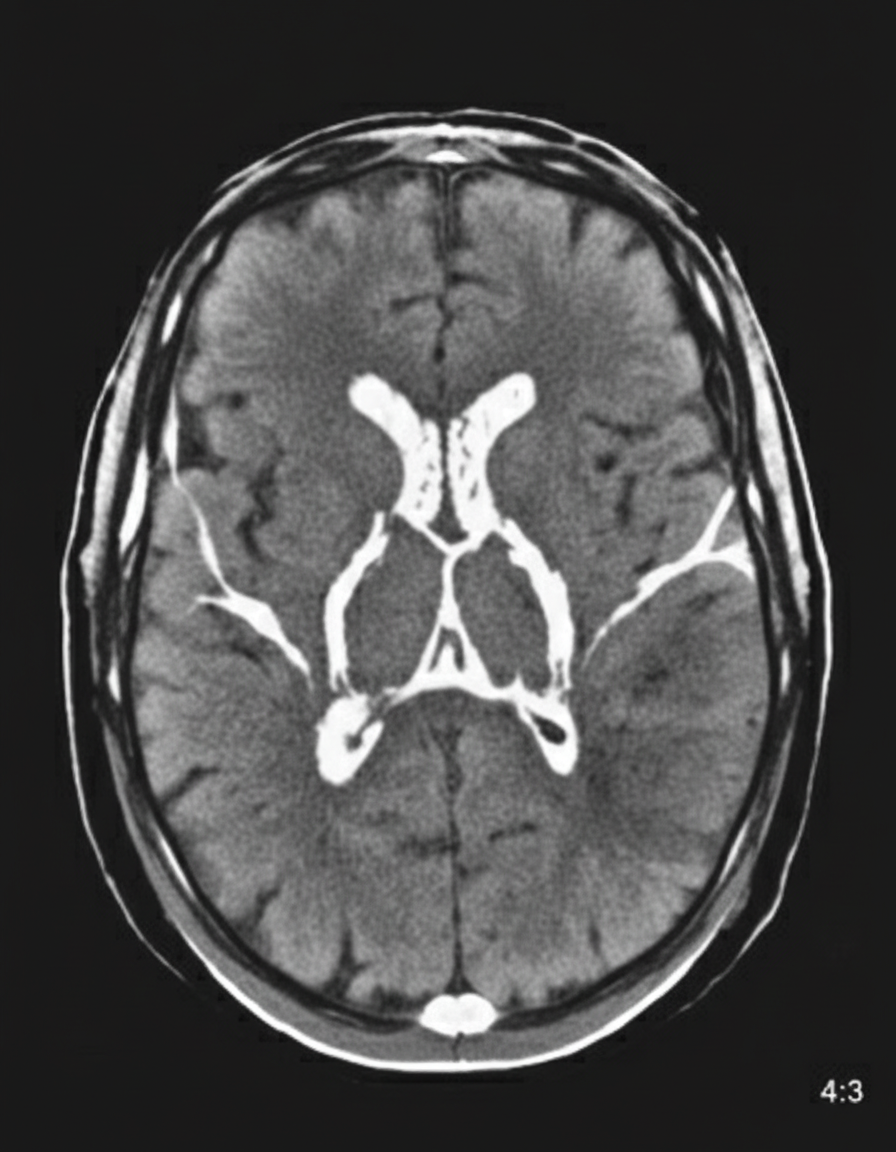
A 48-year-old woman is brought to the emergency department because of a 1-hour history of sudden-onset headache associated with nausea and vomiting. The patient reports she was sitting at her desk when the headache began. The headache is global and radiates to her neck. She has hypertension. She has smoked one pack of cigarettes daily for the last 10 years. She drinks alcohol occasionally. Her father had a stroke at the age 58 years. Current medications include hydrochlorothiazide. She is in severe distress. She is alert and oriented to person, place, and time. Her temperature is 38.2°C (100.8°F), pulse is 89/min, respirations are 19/min, and blood pressure is 150/90 mm Hg. Cardiopulmonary examination shows no abnormalities. Cranial nerves II–XII are intact. She has no focal motor or sensory deficits. She flexes her hips and knees when her neck is flexed while lying in a supine position. A CT scan of the head is shown. Which of the following is the most appropriate intervention?
A 52-year-old man is brought to the emergency department with a 2-hour history of severe, sudden-onset generalized headache. He has since developed nausea and has had one episode of vomiting. The symptoms began while he was at home watching television. Six days ago, he experienced a severe headache that resolved without treatment. He has hypertension and hyperlipidemia. The patient has smoked two packs of cigarettes daily for 30 years. His current medications include lisinopril-hydrochlorothiazide and simvastatin. His temperature is 38.1°C (100.6°F), pulse is 82/min, respirations are 16/min, and blood pressure is 162/98 mm Hg. The pupils are equal, round, and reactive to light. Fundoscopic examination shows no swelling of the optic discs. Cranial nerves II–XII are intact. He has no focal motor or sensory deficits. Finger-to-nose and heel-to-shin testing are normal. A CT scan of the head shows no abnormalities. Which of the following is the most appropriate next step in management?
A 56-year-old woman presents with sudden-onset severe headache, nausea, vomiting, and neck pain for the past 90 minutes. She describes her headache as a ‘thunderclap’, followed quickly by severe neck pain and stiffness, nausea and vomiting. She denies any loss of consciousness, seizure, or similar symptoms in the past. Her past medical history is significant for an episode 6 months ago where she suddenly had trouble putting weight on her right leg, which resolved within hours. The patient denies any history of smoking, alcohol or recreational drug use. On physical examination, the patient has significant nuchal rigidity. Her muscle strength in the lower extremities is 4/5 on the right and 5/5 on the left. The remainder of the physical examination is unremarkable. A noncontrast CT scan of the head is normal. Which of the following is the next best step in the management of this patient?
A 17-year-old boy is brought to the emergency department by his brother after losing consciousness 1 hour ago. The brother reports that the patient was skateboarding outside when he fell on the ground and started to have generalized contractions. There was also some blood coming from his mouth. The contractions stopped after about 1 minute, but he remained unconscious for a few minutes afterward. He has never had a similar episode before. There is no personal or family history of serious illness. He does not smoke or drink alcohol. He does not use illicit drugs. He takes no medications. On arrival, he is confused and oriented only to person and place. He cannot recall what happened and reports diffuse muscle ache, headache, and fatigue. He appears pale. His temperature is 37°C (98.6°F), pulse is 80/min, and blood pressure is 130/80 mm Hg. There is a small wound on the left side of the tongue. A complete blood count and serum concentrations of electrolytes, urea nitrogen, and creatinine are within the reference ranges. Toxicology screening is negative. An ECG shows no abnormalities. Which of the following is the most appropriate next step in management?
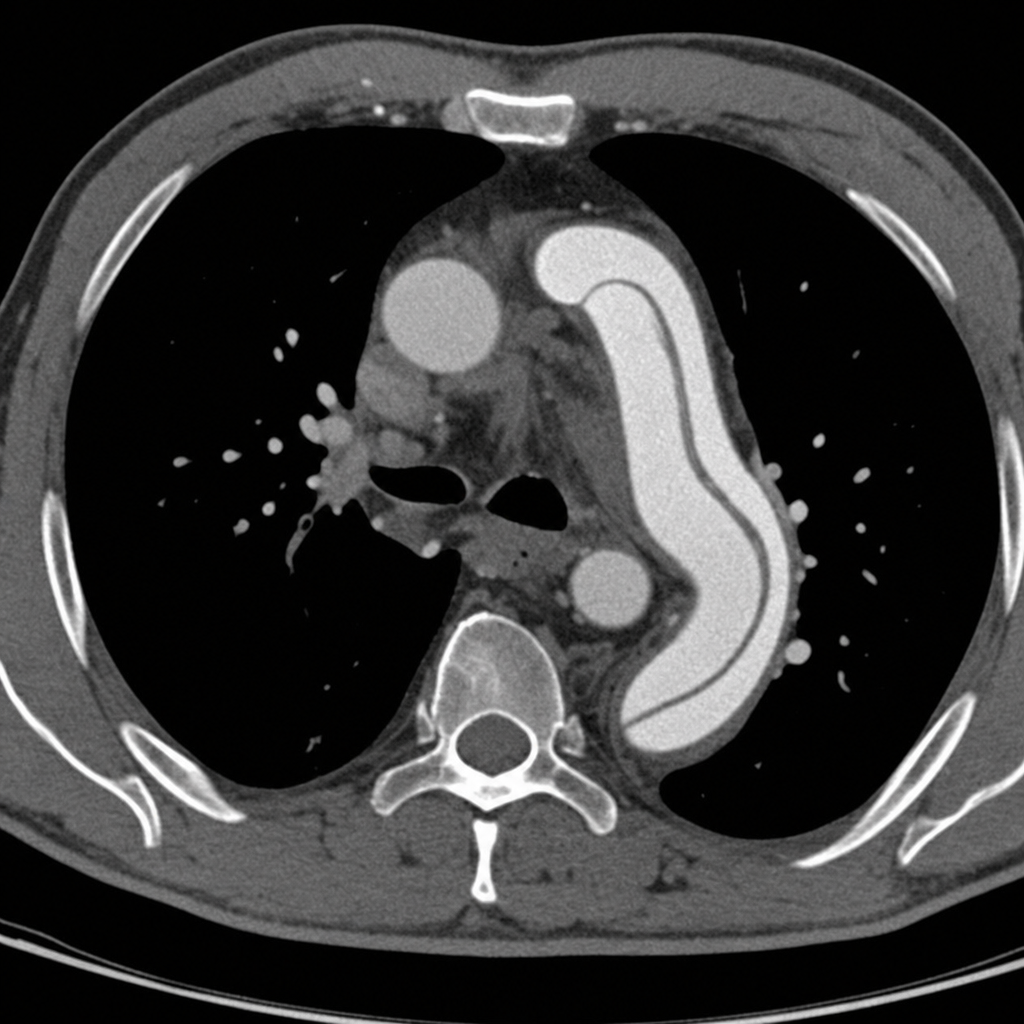
A 67-year-old man with a history of hypertension and a 40 pack-year smoking history presents to the emergency department with sudden onset of tearing chest pain radiating to his back. His blood pressure is 180/100 mmHg in the right arm and 142/88 mmHg in the left arm. A CT angiogram of the chest is obtained and demonstrates an intimal flap in the descending thoracic aorta originating distal to the left subclavian artery, with no involvement of the ascending aorta. Based on this finding, which of the following is the most appropriate next step in management?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app