
Neurosurgery Basics — MCQs

On this page
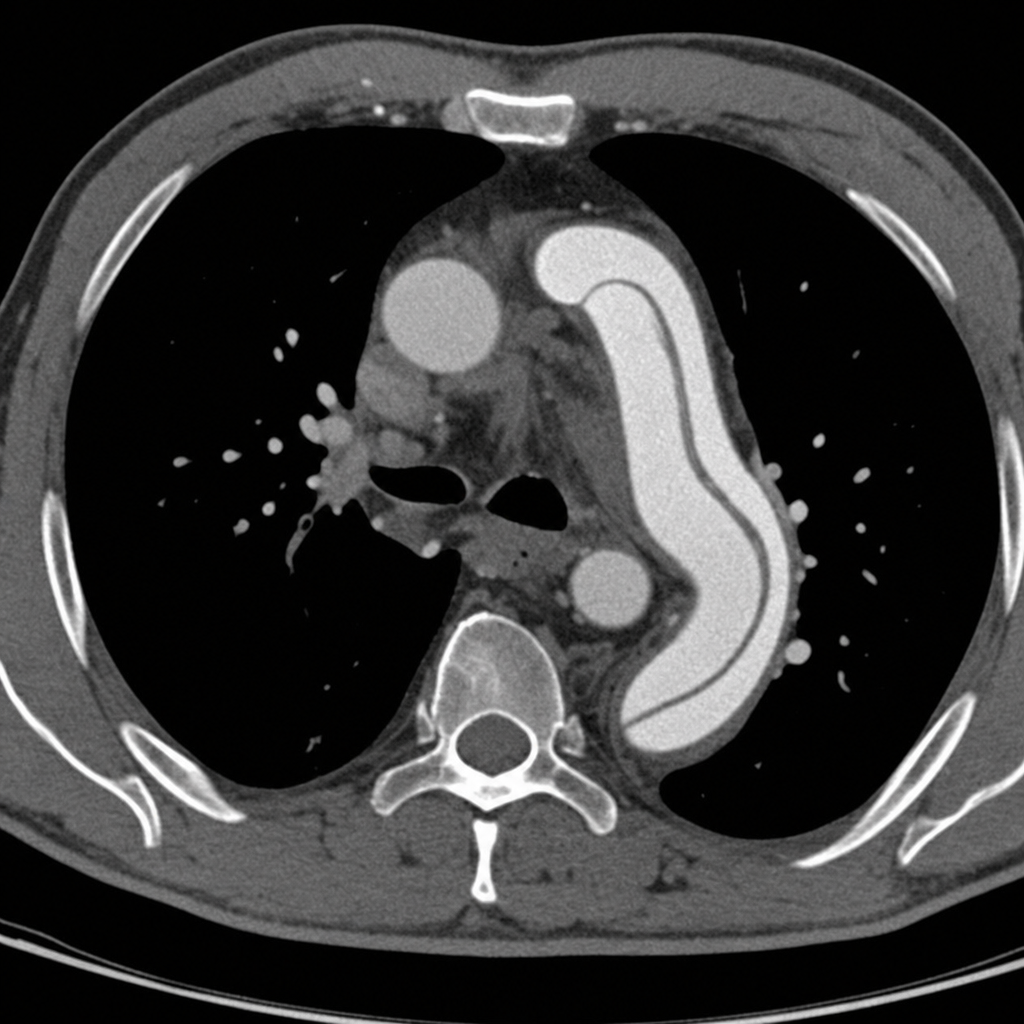
A 67-year-old man with a history of hypertension and a 40 pack-year smoking history presents to the emergency department with sudden onset of tearing chest pain radiating to his back. His blood pressure is 180/100 mmHg in the right arm and 142/88 mmHg in the left arm. A CT angiogram of the chest is obtained and demonstrates an intimal flap in the descending thoracic aorta originating distal to the left subclavian artery, with no involvement of the ascending aorta. Based on this finding, which of the following is the most appropriate next step in management?
A 48-year-old woman undergoes awake craniotomy for resection of a left frontal glioma near Broca's area. Intraoperatively, cortical mapping identifies eloquent tissue, but the tumor extends into functionally critical regions. The surgeon achieves 70% resection when the patient develops expressive aphasia during mapping. Frozen section shows low-grade astrocytoma. The family previously expressed desire for maximal resection. Evaluate the intraoperative decision-making.
A 25-year-old man with newly diagnosed glioblastoma multiforme undergoes gross total resection. Pathology confirms IDH-wild type, MGMT promoter unmethylated tumor. His parents want aggressive treatment, but oncology notes poor prognosis (median survival 12-15 months). The patient is engaged to be married and wants to prioritize quality of life. Radiation oncology recommends standard chemoradiation. Evaluate the most appropriate management approach considering prognostic factors and patient values.
A 70-year-old man with atrial fibrillation on warfarin falls down stairs and presents with severe headache. CT shows a 50 mL acute subdural hematoma with 6 mm midline shift. His INR is 3.8, platelet count 180,000/μL, and GCS is 13. He is moving all extremities. Neurosurgery recommends evacuation, but anesthesia is concerned about reversal timing affecting surgical bleeding. Evaluate the optimal coagulation management strategy.
A 40-year-old woman undergoes transsphenoidal resection of a pituitary macroadenoma. On postoperative day 3, she develops polyuria (6 liters/day), serum sodium of 152 mEq/L, urine specific gravity of 1.002, and serum osmolality of 310 mOsm/kg. After desmopressin administration, her urine output normalizes and sodium improves. On day 7, she develops hyponatremia (128 mEq/L) with concentrated urine. Analyze the underlying pathophysiology.
A 5-year-old boy presents with morning headaches, vomiting, and ataxia. MRI shows a 5 cm enhancing posterior fossa mass arising from the fourth ventricle with hydrocephalus. During preoperative evaluation, he develops acute altered mental status and upward gaze palsy. Vital signs show blood pressure 140/90 mmHg, heart rate 50 bpm, respiratory rate 10/min. Analyze the pathophysiology and appropriate intervention.
A 62-year-old man presents with progressive right arm weakness and difficulty walking. MRI shows a 3 cm intra-axial ring-enhancing lesion in the left motor cortex with significant perilesional edema. He has a 40 pack-year smoking history. Chest CT reveals a 4 cm spiculated left upper lobe lung mass and multiple bilateral pulmonary nodules. Brain biopsy confirms metastatic adenocarcinoma. Analyze the most appropriate neurosurgical management.
A 32-year-old woman with a known 8 mm unruptured cerebral aneurysm of the middle cerebral artery presents for surgical consultation. She is asymptomatic, has no family history of aneurysmal rupture, is a non-smoker, and works as a software engineer. She asks about treatment options. Apply evidence-based counseling regarding management.
A 55-year-old man undergoes elective lumbar laminectomy for spinal stenosis. On postoperative day 2, he develops severe back pain at the surgical site, fever of 39.2°C, and a small amount of purulent drainage from the wound. His WBC count is 18,000/μL. MRI shows fluid collection in the epidural space with rim enhancement. Apply the appropriate management strategy.
A 28-year-old woman presents with progressively worsening headaches, papilledema, and a CT scan showing a 4 cm solid and cystic mass in the posterior fossa with obstructive hydrocephalus. Her symptoms have worsened over the past 24 hours with increasing drowsiness. Apply the most appropriate initial surgical management.
Practice by Chapter
Arteriovenous malformation treatment
Practice Questions
Brain tumor classification and management
Practice Questions
Cerebral aneurysm management
Practice Questions
Craniotomy indications and techniques
Practice Questions
Hydrocephalus diagnosis and shunt procedures
Practice Questions
Intracranial pressure management
Practice Questions
Lumbar puncture technique and indications
Practice Questions
Peripheral nerve surgery basics
Practice Questions
Spinal cord injury management
Practice Questions
Spinal fusion procedures
Practice Questions
Spinal surgery fundamentals
Practice Questions
Stereotactic procedures
Practice Questions
Subdural and epidural hematoma management
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app