
Pelvic organ prolapse repair — MCQs

A 37-year-old woman presents with an inability to void in the hours after giving birth to her first child via vaginal delivery. Her delivery involved the use of epidural anesthesia as well as pelvic trauma from the use of forceps. She is currently experiencing urinary leakage and complains of increased lower abdominal pressure. Which of the following is the most appropriate treatment for this patient’s condition?
A 36-year-old woman comes to the physician for a 2-month history of urinary incontinence and a vaginal mass. She has a history of five full-term normal vaginal deliveries. She gave birth to a healthy newborn 2-months ago. Since then she has felt a sensation of vaginal fullness and a firm mass in the lower vagina. She has loss of urine when she coughs, sneezes, or exercises. Pelvic examination shows an irreducible pink globular mass protruding out of the vagina. A loss of integrity of which of the following ligaments is most likely involved in this patient's condition?
A 61-year-old G4P3 presents with a 5-year history of involuntary urine loss on coughing, sneezing, and physical exertion. She denies urine leakage at night. She has been menopausal since 51 years of age. She is otherwise healthy and is not on any medications, including hormone replacement therapy. The weight is 78 kg (172 lb) and the height is 156 cm (5.1 ft). The vital signs are within normal limits. The physical examination shows no costovertebral angle tenderness. The neurologic examination is unremarkable. The gynecologic examination revealed pale and thin vulvar and vaginal mucosa. The external urethral opening appears normal; there is urine leakage when the patient is asked to cough. The Q-tip test is positive. The bimanual exam reveals painless bulging of the anterior vaginal wall. Which of the following findings are most likely to be revealed by cystometry?
A 63-year-old woman visits her family physician because she has been experiencing difficulty to get her urine stream started in the past 8 months with many occasions needing extra effort to pass the urine. She describes the stream as intermittent and slow, and comments that she needs to go to the restroom again immediately after urinating. Her personal medical history is negative for malignancies, and all of her cytologies have been reported as normal. The only medication she takes is an angiotensin receptor blocker to treat essential hypertension diagnosed 5 years ago. Physical examination is unremarkable except for herniation of the anterior wall of the vagina that goes beyond the hymen. Which of the following types of incontinence is affecting the patient?
A 66-year-old G3P3 presents with an 8-year-history of back pain, perineal discomfort, difficulty urinating, recurrent malaise, and low-grade fevers. These symptoms have recurred regularly for the past 5–6 years. She also says that there are times when she experiences a feeling of having a foreign body in her vagina. With the onset of symptoms, she was evaluated by a physician who prescribed her medications after a thorough examination and recommended a vaginal pessary, but she was non-compliant. She had 3 vaginal deliveries She has been menopausal since 51 years of age. She does not have a history of malignancies or cardiovascular disease. She has type 2 diabetes mellitus that is controlled with diet and metformin. Her vital signs include: blood pressure 110/60 mm Hg, heart rate 91/min, respiratory rate 13/min, and temperature 37.4℃ (99.3℉). On physical examination, there is bilateral costovertebral angle tenderness. The urinary bladder is non-palpable. The gynecologic examination reveals descent of the cervix to the level of the introitus. A Valsalva maneuver elicits uterine procidentia. Which pathology is most likely to be revealed by imaging in this patient?
A 45-year-old man undergoes elective vasectomy for permanent contraception. The procedure is performed under local anesthesia. There are no intra-operative complications and he is discharged home with ibuprofen for post-operative pain. This patient is at increased risk for which of the following complications?
A previously healthy 20-year-old woman comes to her physician because of pain during sexual intercourse. She recently became sexually active with her boyfriend. She has had no other sexual partners. She is frustrated because she has consistently been experiencing a severe, sharp vaginal pain on penetration. She has tried lubricants without significant relief. She has not been able to use tampons in the past due to similar pain with tampon insertion. External vulvar examination shows no abnormalities. She is unable to undergo a bimanual or speculum exam due to intracoital pain with attempted digit or speculum insertion. Testing for Chlamydia trachomatis and Neisseria gonorrhoeae is negative. Which of the following is the best next step in management?
A 63-year-old woman presents to her primary care doctor with increased urinary frequency. She has noticed that over the past 6 months, she has had to urinate more often than usual. Several times per day, she develops a rapid-onset need to urinate and has occasionally been unable to reach the restroom. These symptoms have caused her a lot of distress and impacted her work as a grocery store clerk. She has tried pelvic floor exercises, decreasing her caffeine consumption, and has intentionally lost 20 pounds in an effort to alleviate her symptoms. She denies urinary hesitancy or hematuria. Her past medical history is notable for rheumatoid arthritis for which she takes methotrexate. She does not smoke or drink alcohol. Her temperature is 98.8°F (37.1°C), blood pressure is 124/68 mmHg, pulse is 89/min, and respirations are 19/min. She is well-appearing and in no acute distress. Which of the following interventions would be most appropriate in this patient?
A 77-year-old woman, gravida 2, para 2, is brought to the physician by staff of the nursing home where she resides because of involuntary loss of urine and increased frequency of urination over the past 2 weeks. She reports that she has very little time to get to the bathroom after feeling the urge to urinate. “Accidents” have occurred 4–6 times a day during this period. She has never had urinary incontinence before. She has also been more tired than usual. She drinks 3 cups of coffee daily. Her last menstrual period was 15 years ago. She takes no medications. Vital signs are within normal limits. The abdomen is soft and nontender. Pelvic examination shows a normal-appearing vagina and cervix; uterus and adnexa are small. Which of the following is the most appropriate next step in management?
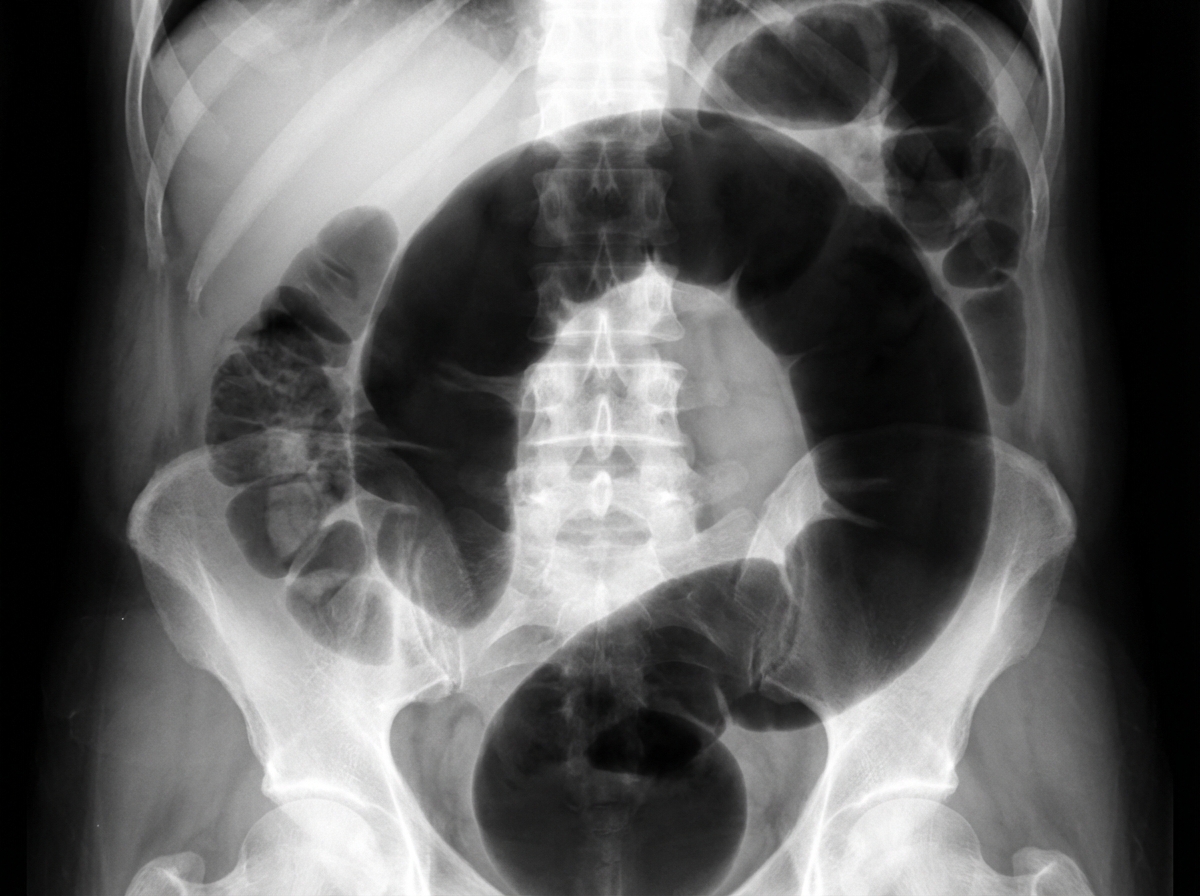
An institutionalized 65-year-old man is brought to the emergency department because of abdominal pain and distension for 12 hours. The pain was acute in onset and is a cramping-type pain associated with nausea, vomiting, and constipation. He has a history of chronic constipation and has used laxatives for years. There is no history of inflammatory bowel disease in his family. He has not been hospitalized recently. There is no recent history of weight loss or change in bowel habits. On physical examination, the patient appears ill. The abdomen is distended with tenderness mainly in the left lower quadrant and is tympanic on percussion. The blood pressure is 110/79 mm Hg, heart rate is 100/min, the respiratory rate is 20/min, and the temperature is 37.2°C (99.0°F). The CBC shows an elevated white blood cell count. The plain abdominal X-ray is shown in the accompanying image. What is the most likely cause of his condition?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app