
Small bowel resection and anastomosis — MCQs

A 72-year-old female presents to the emergency department complaining of severe abdominal pain and several days of bloody diarrhea. Her symptoms began with intermittent bloody diarrhea five days ago and have worsened steadily. For the last 24 hours, she has complained of fevers, chills, and abdominal pain. She has a history of ulcerative colitis, idiopathic hypertension, and hypothyroidism. Her medications include hydrochlorothiazide, levothyroxine, and sulfasalazine. In the ED, her temperature is 39.1°C (102.4°F), pulse is 120/min, blood pressure is 90/60 mmHg, and respirations are 20/min. On exam, the patient is alert and oriented to person and place, but does not know the day. Her mucus membranes are dry. Heart and lung exam are not revealing. Her abdomen is distended with marked rebound tenderness. Bowel sounds are hyperactive. Serum: Na+: 142 mEq/L Cl-: 107 mEq/L K+: 3.3 mEq/L HCO3-: 20 mEq/L BUN: 15 mg/dL Glucose: 92 mg/dL Creatinine: 1.2 mg/dL Calcium: 10.1 mg/dL Hemoglobin: 11.2 g/dL Hematocrit: 30% Leukocyte count: 14,600/mm^3 with normal differential Platelet count: 405,000/mm^3 What is the next best step in management?
A 69-year-old male presents to the Emergency Department with bilious vomiting that started within the past 24 hours. His medical history is significant for hypertension, hyperlipidemia, and a myocardial infarction six months ago. His past surgical history is significant for a laparotomy 20 years ago for a perforated diverticulum. Most recently he had some dental work done and has been on narcotic pain medicine for the past week. He reports constipation and obstipation. He is afebrile with a blood pressure of 146/92 mm Hg and a heart rate of 116/min. His abdominal exam reveals multiple well-healed scars with distension but no tenderness. An abdominal/pelvic CT scan reveals dilated small bowel with a transition point to normal caliber bowel distally. When did the cause of his pathology commence?
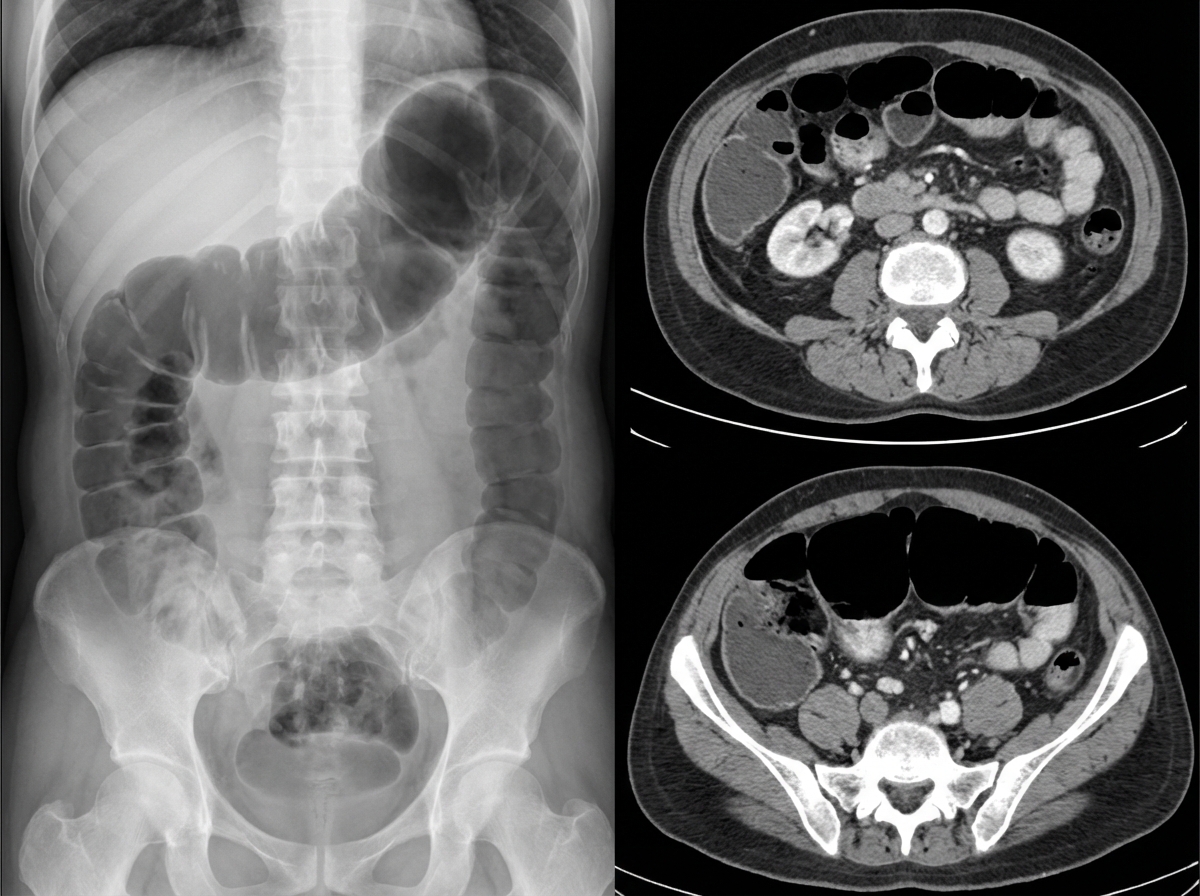
A 76-year-old female is brought to the emergency department after being found unresponsive in her room at her nursing facility. Past medical history is significant for Alzheimer's disease, hypertension, and diabetes. Surgical history is notable for an open cholecystectomy at age 38 and multiple cesarean sections. On arrival, she is non-responsive but breathing by herself, and her vital signs are T 102.9 F, HR 123 bpm, BP 95/64, RR 26/min, and SaO2 97% on 6L nasal cannula. On physical exam the patient has marked abdominal distension and is tympanic to percussion. Laboratory studies are notable for a lactic acidosis. An upright abdominal radiograph and CT abdomen/pelvis with contrast are shown in Figures A and B respectively. She is started on IV fluids and a nasogastric tube is placed to suction which returns green bilious fluid. Repeat vitals 1 hour later are T 101F, HR 140 bpm, BP 75/44, RR 30/min, and SaO2 is 100% on the ventilator after she is intubated for airway concerns. What is the next best step in management?
A 64-year-old woman has progressively worsening abdominal pain 5 hours after an open valve replacement with cardiopulmonary bypass. The pain is crampy and associated with an urge to defecate. The patient reports having had 2 bloody bowel movements in the last hour. Her operation was complicated by significant intraoperative blood loss, which prolonged the operation and necessitated 2 transfusions of red blood cells. She has hypercholesterolemia and type 2 diabetes mellitus. The patient received prophylactic perioperative antibiotics and opioid pain management during recovery. Her temperature is 37.9°C (98.9°F), pulse is 95/min, and blood pressure is 115/69 mm Hg. Examination shows a soft abdomen with mild tenderness to palpation in the left quadrants but no rebound tenderness or guarding. Bowel sounds are decreased. Rectal examination shows blood on the examining finger. Which of the following is the most likely underlying cause of this patient's symptoms?
A 47-year-old woman presents to the emergency department with abdominal pain. The patient states that she felt this pain come on during dinner last night. Since then, she has felt bloated, constipated, and has been vomiting. Her current medications include metformin, insulin, levothyroxine, and ibuprofen. Her temperature is 99.0°F (37.2°C), blood pressure is 139/79 mmHg, pulse is 95/min, respirations are 12/min, and oxygen saturation is 98% on room air. On physical exam, the patient appears uncomfortable. Abdominal exam is notable for hypoactive bowel sounds, abdominal distension, and diffuse tenderness in all four quadrants. Cardiac and pulmonary exams are within normal limits. Which of the following is the best next step in management?
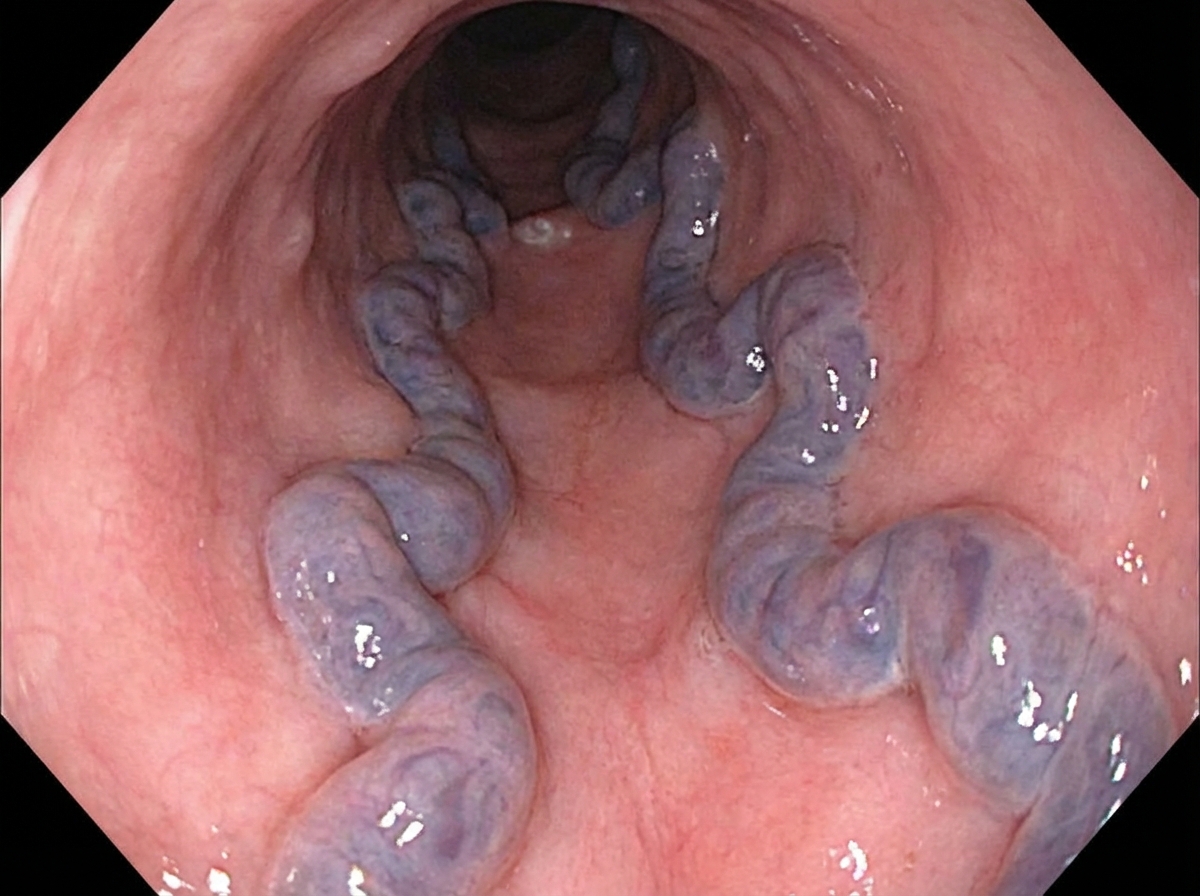
A 55-year-old man is brought to the emergency department by his friends after he was found vomiting copious amounts of blood. According to his friends, he is a chronic alcoholic and lost his family and job because of his drinking. The admission vital signs were as follows: blood pressure is 100/75 mm Hg, heart rate is 95/min, respiratory rate is 15/min, and oxygen saturation is 97% on room air. He is otherwise alert and oriented to time, place, and person. The patient was stabilized with intravenous fluids and a nasogastric tube was inserted. He is urgently prepared for endoscopic evaluation. An image from the procedure is shown. Which of the following sets of pathologies with the portacaval anastomoses is paired correctly?
Four days after undergoing a total abdominal hysterectomy for atypical endometrial hyperplasia, a 59 year-old woman reports abdominal bloating and discomfort. She has also had nausea without vomiting. She has no appetite despite not having eaten since the surgery and drinking only sips of water. Her postoperative pain has been well controlled on a hydromorphone patient-controlled analgesia (PCA) pump. Her foley was removed on the second postoperative day and she is now voiding freely. Although she lays supine in bed for most of the day, she is able to walk around the hospital room with a physical therapist. Her temperature is 36.5°C (97.7°F), pulse is 84/min, respirations are 10/min, and blood pressure is 132/92 mm Hg. She is 175 cm (5 ft 9 in) tall and weighs 115 kg (253 lb); BMI is 37.55 kg/m2. Examination shows a mildly distended, tympanic abdomen; bowel sounds are absent. Laboratory studies are within normal limits. An x-ray of the abdomen shows uniform distribution of gas in the small bowel, colon, and rectum without air-fluid levels. Which of the following is the most appropriate next step in the management of this patient?
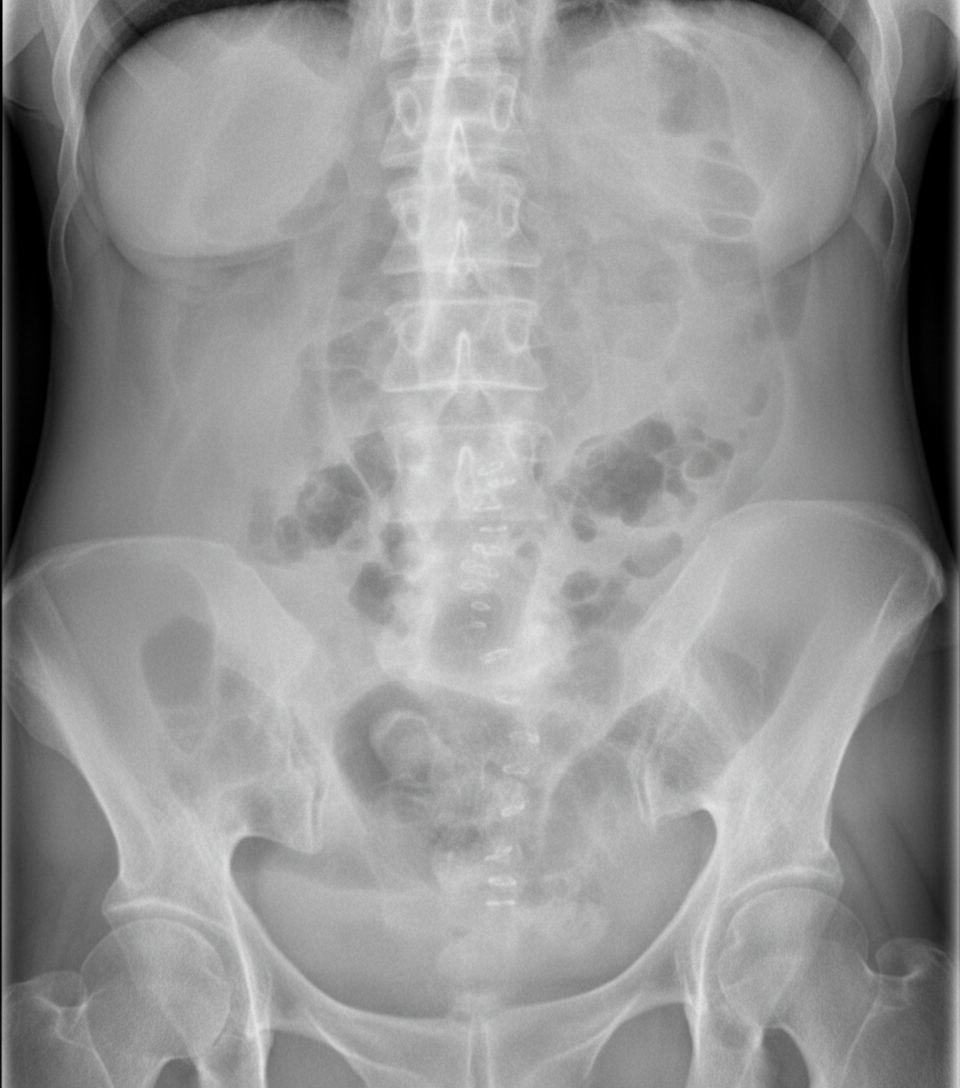
A 14-year-old boy is brought to the emergency department because of abdominal swelling and vomiting over the past 24 hours. He has generalized abdominal pain. He has no history of any serious illnesses and takes no medications. His temperature is 36.7°C (98.1°F), blood pressure is 115/70 mm/Hg, pulse is 88/min, and respirations are 16/min. Abdominal examination shows diffuse swelling with active bowel sounds. Mild generalized tenderness without guarding or rebound is noted. His leukocyte count is 8,000/mm3. An X-ray of the abdomen is shown. Intravenous fluids have been initiated. Which of the following is the most appropriate next step in management?
One day after undergoing an open colectomy, a 65-year-old man with colon cancer experiences shivers. The procedure was originally scheduled to be done laparoscopically, but it was converted because of persistent bleeding. Besides the conversion, the operation was uneventful. Five years ago, he underwent renal transplantation because of cystic disease and has been taking prednisolone since then. He has a history of allergy to sulfonamides. He appears acutely ill. His temperature is 39.2°C (102.5°F), pulse is 120/min, respirations are 23/min, and blood pressure is 90/62 mm Hg. Abdominal examination shows a midline incision extending from the xiphisternum to the pubic symphysis. There is a 5-cm (2-in) area of purplish discoloration near the margin of the incision in the lower abdomen. Palpation of the abdomen produces severe pain and crackling sounds are heard. Laboratory studies show: Hemoglobin 12.5 g/dL Leukocyte count 18,600/mm3 Platelet count 228,000/mm3 Erythrocyte sedimentation rate 120 mm/h Serum Na+ 134 mEq/L K+ 3.5 mEq/L Cl- 98 mEq/L HCO3- 22 mEq/L Glucose 200 mg/dL Urea nitrogen 60 mg/dL Creatinine 3.2 mg/dL Creatine kinase 750 U/L Which of the following is the most appropriate next step in management?
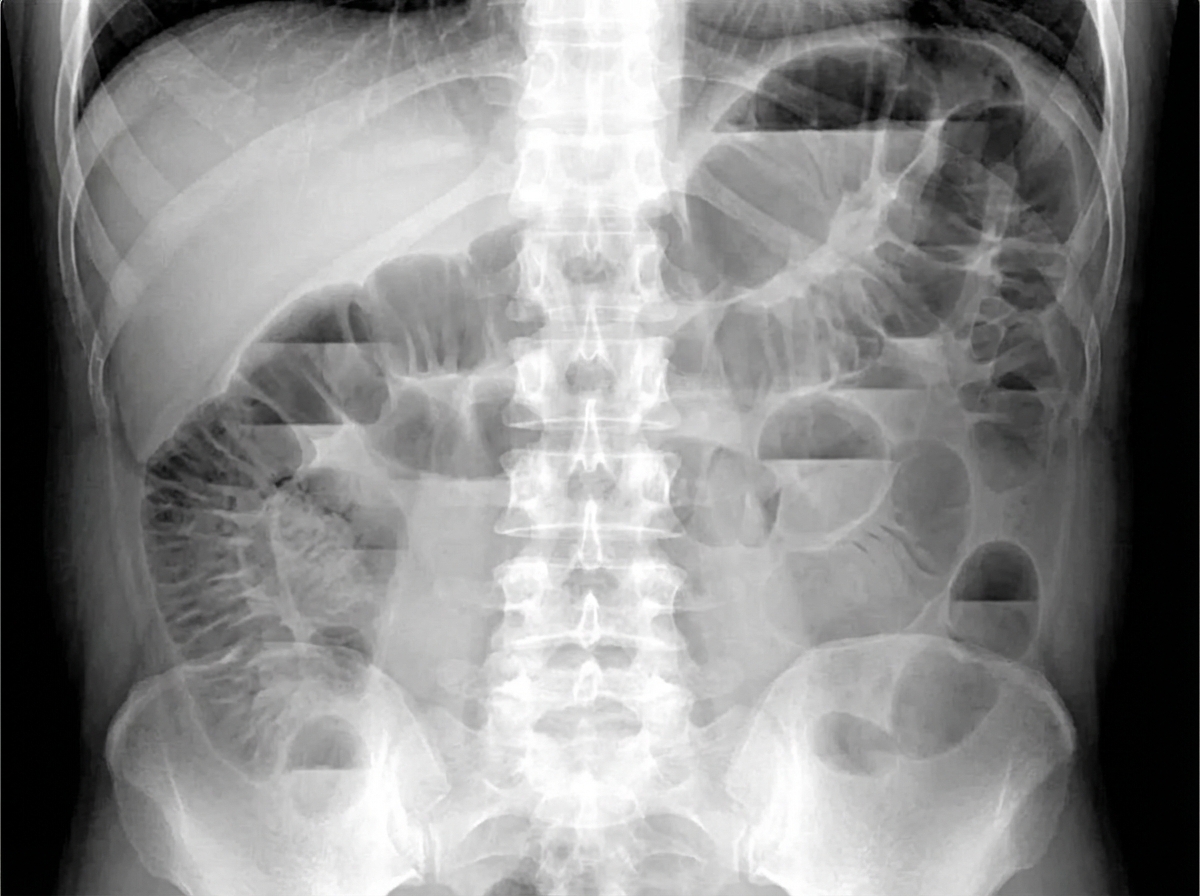
A 75-year-old man is brought to the emergency department after 2 days of severe diffuse abdominal pain, nausea, vomiting, and lack of bowel movements, which has led him to stop eating. He has a history of type-2 diabetes mellitus, hypertension, and chronic obstructive pulmonary disease. Upon admission, his vital signs are within normal limits and physical examination shows diffuse abdominal tenderness, distention, lack of bowel sounds, and an empty rectal ampulla. After initial fluid therapy and correction of moderate hypokalemia, the patient's condition shows mild improvement. His abdominal plain film is taken and shown. Which of the following is the most appropriate concomitant approach?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app