
Esophageal surgery procedures — MCQs

A 23-year-old college senior visits the university health clinic after vomiting large amounts of blood. He has been vomiting for the past 36 hours after celebrating his team’s win at the national hockey championship with his varsity friends while consuming copious amounts of alcohol. His personal medical history is unremarkable. His blood pressure is 129/89 mm Hg while supine and 100/70 mm Hg while standing. His pulse is 98/min, strong and regular, with an oxygen saturation of 98%. His body temperature is 36.5°C (97.7°F), while the rest of the physical exam is normal. Which of the following is associated with this patient’s condition?
A previously healthy 55-year-old man comes to the physician because of a 5-month history of progressively worsening substernal chest pain after meals. The pain occurs almost daily, is worst after eating spicy food or drinking coffee, and often wakes him up from sleep at night. He has not had any weight loss. He has smoked 1 pack of cigarettes daily for 35 years and he drinks 1 to 2 glasses of wine daily with dinner. Physical examination is unremarkable. Esophagogastroduodenoscopy shows erythema of the distal esophagus with two small mucosal erosions. Biopsy specimens obtained from the esophagus show no evidence of metaplasia. Without treatment, this patient is at greatest risk for which of the following complications?
A 58-year-old man comes to the physician for the evaluation of intermittent dysphagia for 6 months. He states that he drinks a lot of water during meals to help reduce discomfort he has while swallowing food. He has hypertension and gastroesophageal reflux disease. He has smoked one half-pack of cigarettes daily for 32 years. He does not drink alcohol. Current medications include hydrochlorothiazide and ranitidine. He is 173 cm (5 ft 8 in) tall and weighs 101 kg (222 lb); BMI is 33.7 kg/m2. His temperature is 37°C (98.6°F), pulse is 75/min, and blood pressure is 125/75 mm Hg. The lungs are clear to auscultation. Cardiac examination shows no murmurs, rubs, or gallops. The abdomen is soft and nontender. A barium esophagogram shows a smooth, circumferential narrowing at the distal esophagus. An upper endoscopy shows a sliding hiatal hernia and a thin mucosal ring at the gastroesophageal junction. Biopsies from the area show normal squamous and columnar epithelium with no dysplasia or malignancy. Which of the following is the most appropriate next step in the management of this patient?
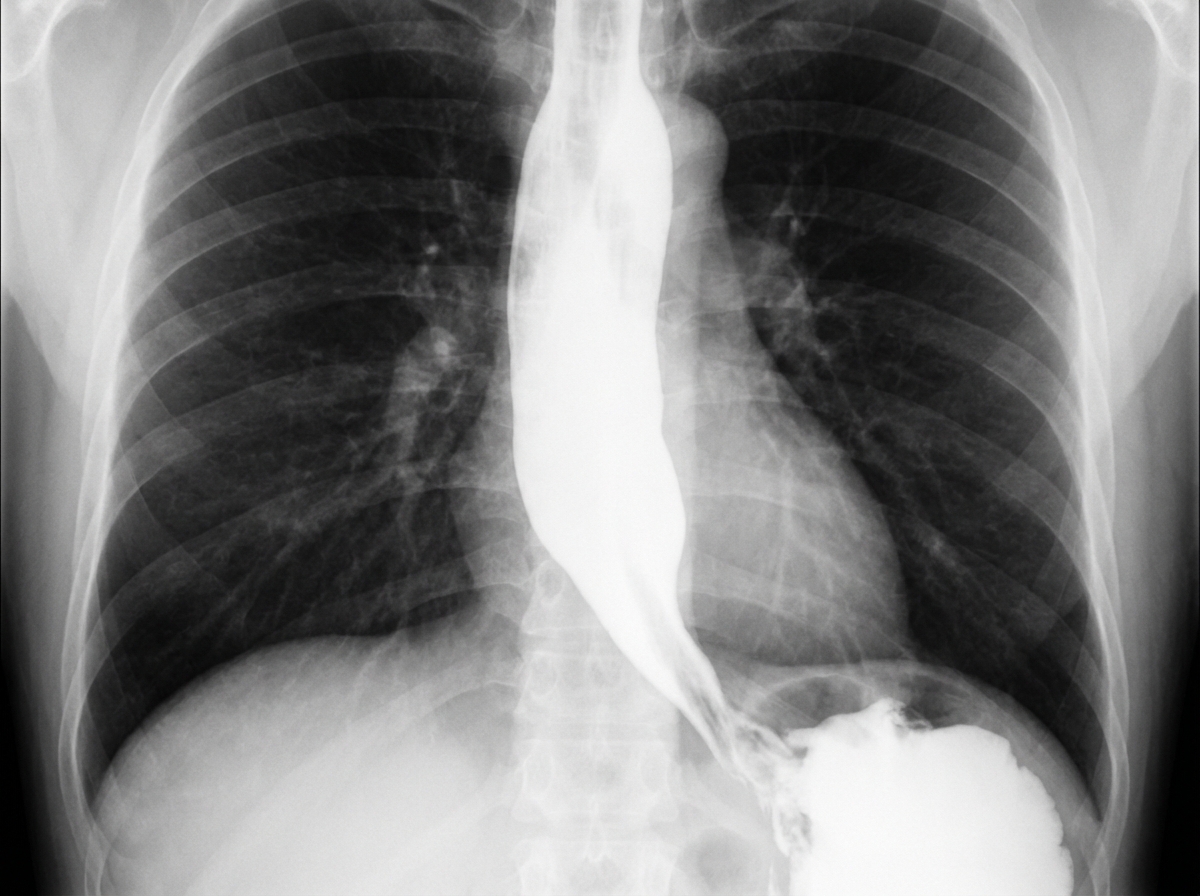
A 62-year-old man is referred to a gastroenterologist because of difficulty swallowing for the past 5 months. He has difficulty swallowing both solid and liquid foods, but there is no associated pain. He denies any shortness of breath or swelling in his legs. He immigrated from South America 10 years ago. He is a non-smoker and does not drink alcohol. His physical examination is unremarkable. A barium swallow study was ordered and the result is given below. Esophageal manometry confirms the diagnosis. What is the most likely underlying cause of this patient’s condition?
A 58-year-old man comes to the physician for recurrent heartburn for 12 years. He has also developed a cough for a year, which is worse at night. He has smoked a pack of cigarettes daily for 30 years. His only medication is an over-the-counter antacid. He has not seen a physician for 8 years. He is 175 cm (5 ft 9 in) tall and weighs 95 kg (209 lb); BMI is 31 kg/m2. Vital signs are within normal limits. There is no lymphadenopathy. The abdomen is soft and nontender. The remainder of the examination shows no abnormalities. A complete blood count is within the reference range. An upper endoscopy shows columnar epithelium 2 cm from the gastroesophageal junction. Biopsies from the columnar epithelium show low-grade dysplasia and intestinal metaplasia. Which of the following is the most appropriate next step in management?
A 63-year-old man presents to the ambulatory medical clinic with symptoms of dysphagia and ‘heartburn’, which he states have become more troublesome over the past year. Past medical history is significant for primary hypertension. On physical exam, he is somewhat tender to palpation over his upper abdomen. The vital signs include: temperature 36.7°C (98.0°F), blood pressure 126/74 mm Hg, heart rate 74/min, and respiratory rate 14/min. Barium swallow fluoroscopy demonstrates a subdiaphragmatic gastroesophageal junction, with herniation of the gastric fundus into the left hemithorax. Given the following options, what is the most appropriate next step in the management of this patient’s underlying condition?
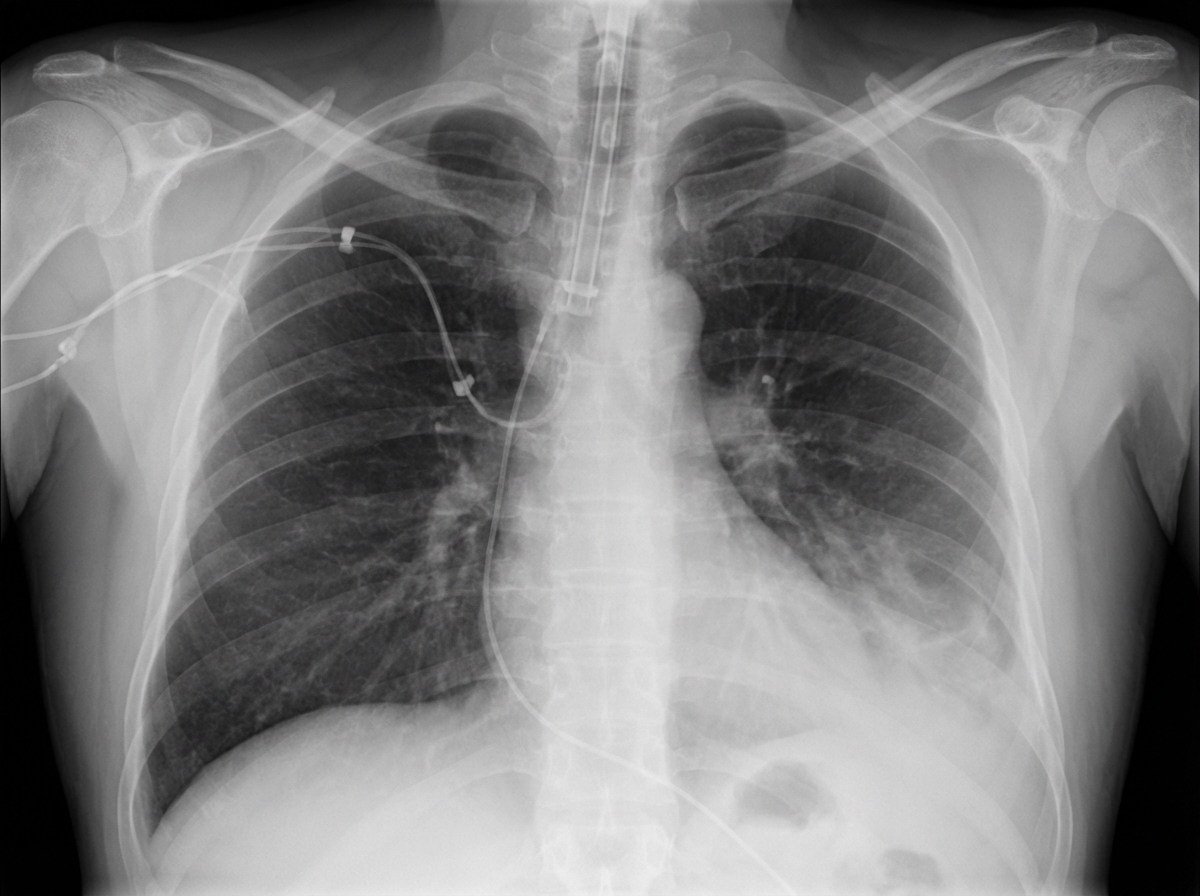
A 63-year-old man is brought to the emergency department, 30 minutes after being involved in a high-speed motor vehicle collision. He is obtunded on arrival. He is intubated and mechanical ventilation is begun. The ventilator is set at a FiO2 of 60%, tidal volume of 440 mL, and positive end-expiratory pressure of 4 cm H2O. On the third day of intubation, his temperature is 37.3°C (99.1°F), pulse is 91/min, and blood pressure is 103/60 mm Hg. There are decreased breath sounds over the left lung base. Cardiac examination shows no abnormalities. The abdomen is soft and not distended. Arterial blood gas analysis shows: pH 7.49 pCO2 29 mm Hg pO2 73 mm Hg HCO3- 20 mEq/L O2 saturation 89% Monitoring shows a sudden increase in the plateau airway pressure. An x-ray of the chest shows deepening of the costophrenic angle on the left side. Which of the following is the most appropriate next step in management?
A 68-year-old man is brought to the emergency department because of fever, progressive weakness, and cough for the past five days. He experienced a similar episode 2 months ago, for which he was hospitalized for 10 days while visiting his son in Russia. He states that he has never fully recovered from that episode. He felt much better after being treated with antibiotics, but he still coughs often during meals. He sometimes also coughs up undigested food after eating. For the last 5 days, his coughing has become more frequent and productive of yellowish-green sputum. He takes hydrochlorothiazide for hypertension and pantoprazole for the retrosternal discomfort that he often experiences while eating. He has smoked half a pack of cigarettes daily for the last 30 years and drinks one shot of vodka every day. The patient appears thin. His temperature is 40.1°C (104.2°F), pulse is 118/min, respirations are 22/min, and blood pressure is 125/90 mm Hg. Auscultation of the lungs shows right basal crackles. There is dullness on percussion at the right lung base. The remainder of the physical examination shows no abnormalities. Laboratory studies show: Hemoglobin 15.4 g/dL Leukocyte count 17,000/mm3 Platelet count 350,000/mm3 Na+ 139 mEq/L K+ 4.6 mEq/L Cl- 102 mEq/L HCO3- 25 mEq/L Urea Nitrogen 16 mg/dL Creatinine 1.3 mg/dL An x-ray of the chest shows a right lower lobe infiltrate. Which of the following is the most likely explanation for this patient's symptoms?
A 68-year-old man comes to the physician because of a 6-month history of difficulty swallowing pieces of meat and choking frequently during meal times. He also sometimes regurgitates foul-smelling, undigested food particles. Examination shows a 3 x 3 cm soft cystic, immobile mass in the upper third of the left side of his neck anterior to the left sternocleidomastoid muscle that becomes prominent when he coughs. A barium swallow shows an accumulation of contrast on the lateral aspect of the neck at the C5 level. Which of the following is the most likely underlying cause for this patient's condition?
A 68-year-old man presents to the office with his wife complaining of difficulty in swallowing, which progressively worsened over the past month. He has difficulty in initiating swallowing and often has to drink water with solid foods. He has no problems swallowing liquids. His wife is concerned about her husband's bad breath. Adding to his wife, the patient mentions a recent episode of vomiting where the vomit smelled 'really bad' and contained the food that he ate 2 days before. On examination, the patient's blood pressure is 110/70 mm Hg, pulse rate is 72/min, with normal bowel sounds, and no abdominal tenderness to palpation. A barium swallow radiograph is performed (shown below), which reveals a localized collection of contrast material in the cervical region suggestive of an outpouching. Which of the following statements best describes the lesion seen on the radiograph?

Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app