
Elective colorectal procedures — MCQs

A 62-year-old man presents to the emergency department with acute pain in the left lower abdomen and profuse rectal bleeding. These symptoms started 3 hours ago. The patient has chronic constipation and bloating, for which he takes lactulose. His family history is negative for gastrointestinal disorders. His temperature is 38.2°C (100.8°F), blood pressure is 90/60 mm Hg, and pulse is 110/min. On physical examination, the patient appears drowsy, and there is tenderness with guarding in the left lower abdominal quadrant. Flexible sigmoidoscopy shows multiple, scattered diverticula with acute mucosal inflammation in the sigmoid colon. Which of the following is the best initial treatment for this patient?
A 26-year-old white man comes to the physician because of increasing generalized fatigue for 6 months. He has been unable to work out at the gym during this period. He has also had cramping lower abdominal pain and diarrhea for the past 5 weeks that is occasionally bloody. His father was diagnosed with colon cancer at the age of 65. He has smoked half a pack of cigarettes daily for the past 10 years. He drinks 1–2 beers on social occasions. His temperature is 37.3°C (99.1°F), pulse is 88/min, and blood pressure is 116/74 mm Hg. Physical examination shows dry mucous membranes. The abdomen is soft and nondistended with slight tenderness to palpation over the lower quadrants bilaterally. Rectal examination shows stool mixed with blood. His hemoglobin concentration is 13.5 g/dL, leukocyte count is 7,500/mm3, and platelet count is 480,000/mm3. Urinalysis is within normal limits. Which of the following is the most appropriate next step in management?
A 64-year-old woman has progressively worsening abdominal pain 5 hours after an open valve replacement with cardiopulmonary bypass. The pain is crampy and associated with an urge to defecate. The patient reports having had 2 bloody bowel movements in the last hour. Her operation was complicated by significant intraoperative blood loss, which prolonged the operation and necessitated 2 transfusions of red blood cells. She has hypercholesterolemia and type 2 diabetes mellitus. The patient received prophylactic perioperative antibiotics and opioid pain management during recovery. Her temperature is 37.9°C (98.9°F), pulse is 95/min, and blood pressure is 115/69 mm Hg. Examination shows a soft abdomen with mild tenderness to palpation in the left quadrants but no rebound tenderness or guarding. Bowel sounds are decreased. Rectal examination shows blood on the examining finger. Which of the following is the most likely underlying cause of this patient's symptoms?
You are a resident in the surgical ICU. One of the patients you are covering is a 35-year-old pregnant G1P0 in her first trimester admitted for complicated appendicitis and awaiting appendectomy. Your attending surgeon would like you to start the patient on moxifloxacin IV preoperatively. You remember from your obstetrics clerkship, however, that moxifloxacin is Pregnancy Category C, and animal studies have shown that immature animals exposed to fluoroquinolones like moxifloxacin may experience cartilage damage. You know that there are potentially safer antibiotics, such as piperacillin/tazobactam, which is in Pregnancy Category B. What should you do?
A 31-year-old woman comes to the emergency department because of a 4-day history of fever and diarrhea. She has abdominal cramps and frequent bowel movements of small quantities of stool with blood and mucus. She has had multiple similar episodes over the past 8 months. Her temperature is 38.1°C (100.6°F), pulse is 75/min, and blood pressure is 130/80 mm Hg. Bowel sounds are normal. The abdomen is soft. There is tenderness to palpation in the left lower quadrant with guarding and no rebound. She receives appropriate treatment and recovers. Two weeks later, colonoscopy shows polypoid growths flanked by linear ulcers. A colonic biopsy specimen shows mucosal edema with distorted crypts and inflammatory cells in the lamina propria. Which of the following is the most appropriate recommendation for this patient?
One day after undergoing an open colectomy, a 65-year-old man with colon cancer experiences shivers. The procedure was originally scheduled to be done laparoscopically, but it was converted because of persistent bleeding. Besides the conversion, the operation was uneventful. Five years ago, he underwent renal transplantation because of cystic disease and has been taking prednisolone since then. He has a history of allergy to sulfonamides. He appears acutely ill. His temperature is 39.2°C (102.5°F), pulse is 120/min, respirations are 23/min, and blood pressure is 90/62 mm Hg. Abdominal examination shows a midline incision extending from the xiphisternum to the pubic symphysis. There is a 5-cm (2-in) area of purplish discoloration near the margin of the incision in the lower abdomen. Palpation of the abdomen produces severe pain and crackling sounds are heard. Laboratory studies show: Hemoglobin 12.5 g/dL Leukocyte count 18,600/mm3 Platelet count 228,000/mm3 Erythrocyte sedimentation rate 120 mm/h Serum Na+ 134 mEq/L K+ 3.5 mEq/L Cl- 98 mEq/L HCO3- 22 mEq/L Glucose 200 mg/dL Urea nitrogen 60 mg/dL Creatinine 3.2 mg/dL Creatine kinase 750 U/L Which of the following is the most appropriate next step in management?
Eight hours after undergoing an open right hemicolectomy and a colostomy for colon cancer, a 52-year-old man has wet and bloody surgical dressings. He has had episodes of blood in his stools during the past 6 months, which led to the detection of colon cancer. He has hypertension and ischemic heart disease. His younger brother died of a bleeding disorder at the age of 16. The patient has smoked one pack of cigarettes daily for 36 years and drinks three to four beers daily. Prior to admission, his medications included aspirin, metoprolol, enalapril, and simvastatin. Aspirin was stopped 7 days prior to the scheduled surgery. He appears uncomfortable. His temperature is 36°C (96.8°F), pulse is 98/min, respirations are 14/min, and blood pressure is 118/72 mm Hg. Examination shows a soft abdomen with a 14-cm midline incision that has severe oozing of blood from its margins. The colostomy bag has some blood collected within. Laboratory studies show: Hemoglobin 12.3 g/dL Leukocyte count 11,200/mm3 Platelet count 210,000/mm3 Bleeding time 4 minutes Prothrombin time 15 seconds (INR=1.1) Activated partial thromboplastin time 36 seconds Serum Urea nitrogen 30 mg/dL Glucose 96 mg/dL Creatinine 1.1 mg/dL AST 48 U/L ALT 34 U/L γ-Glutamyltransferase 70 U/L (N= 5–50 U/L) Which of the following is the most likely cause of this patient's bleeding?
A 38-year-old man comes to the physician because of a 2-week history of severe pain while passing stools. The stools are covered with bright red blood. He has been avoiding defecation because of the pain. Last year, he was hospitalized for pilonidal sinus surgery. He has had chronic lower back pain ever since he had an accident at his workplace 10 years ago. The patient's father was diagnosed with colon cancer at the age of 62. Current medications include oxycodone and gabapentin. He is 163 cm (5 ft 4 in) tall and weighs 100 kg (220 lb); BMI is 37.6 kg/m2. Vital signs are within normal limits. The abdomen is soft and nontender. Digital rectal examination was not performed because of severe pain. His hemoglobin is 16.3 mg/dL and his leukocyte count is 8300/mm3. Which of the following is the most appropriate next step in management?
A 31 year-old-man presents to an urgent care clinic with symptoms of lower abdominal pain, bloating, bloody diarrhea, and fullness, all of which have become more frequent over the last 3 months. Rectal examination reveals a small amount of bright red blood. His vital signs include: temperature 36.7°C (98.0°F), blood pressure 126/74 mm Hg, heart rate 74/min, and respiratory rate 14/min. Colonoscopy is performed, showing extensive mucosal erythema, induration, and pseudopolyps extending from the rectum to the splenic flexure. Given the following options, what is the most appropriate treatment to induce remission in this patient?
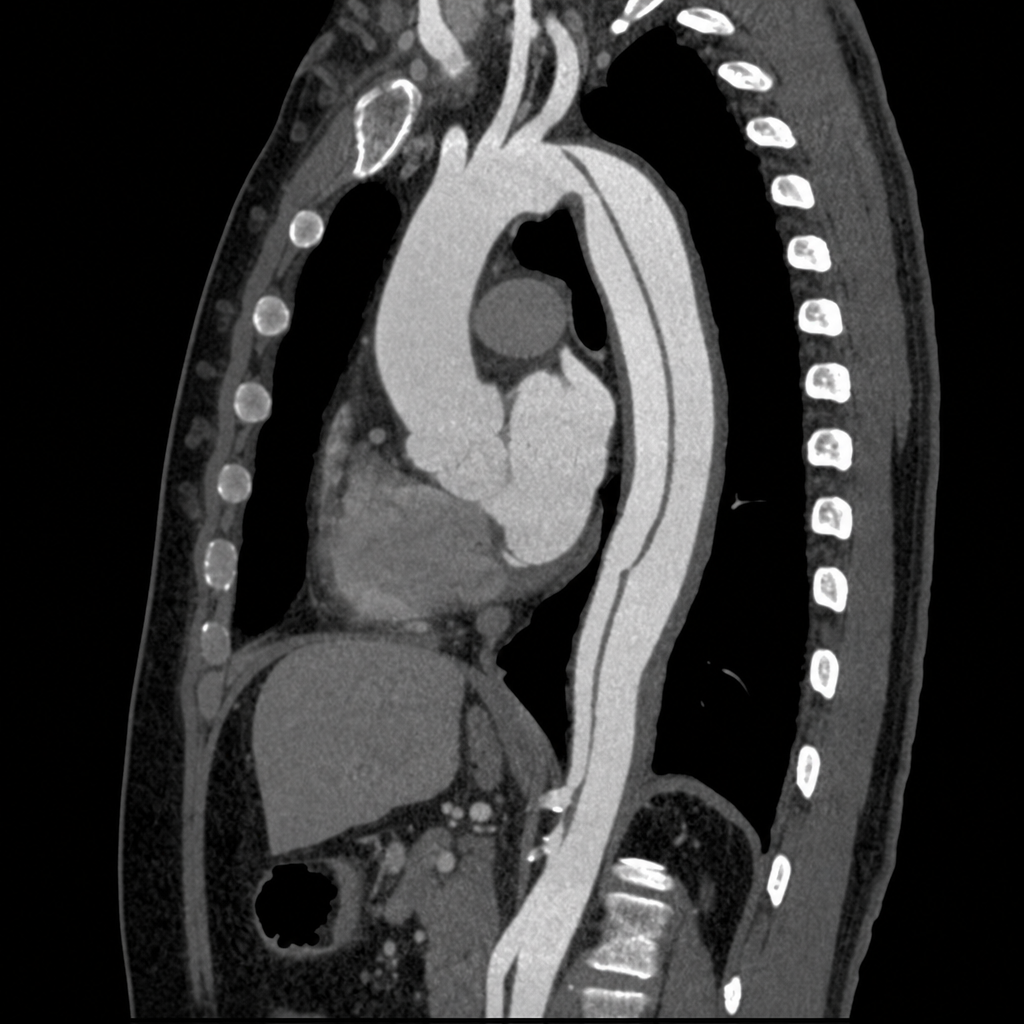
A 55-year-old man presents to the emergency department with sudden-onset tearing chest pain radiating to the interscapular region. He has a history of poorly controlled hypertension. BP is 178/96 mmHg in the right arm and 142/80 mmHg in the left arm. He is diaphoretic and in moderate distress. A CT angiogram of the chest is obtained. The image demonstrates an intimal flap originating 3 cm distal to the left subclavian artery with the false lumen extending through the descending thoracic aorta to the level of the renal arteries; the ascending aorta and aortic root appear normal. Which of the following is the most appropriate management?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app