
Anorectal procedures — MCQs

A 32-year-old woman presents to the office with complaints of intense anal pain every time she has a bowel movement. The pain has been present for the past 4 weeks, and it is dull and throbbing in nature. It is associated with mild bright red bleeding from the rectum that is aggravated during defecation. She has no relevant past medical history. When asked about her sexual history, she reports practicing anal intercourse. The vital signs include heart rate 98/min, respiratory rate 16/min, temperature 37.6°C (99.7°F), and blood pressure 110/66 mm Hg. On physical examination, the anal sphincter tone is markedly increased, and it's impossible to introduce the finger due to severe pain. What is the most likely diagnosis?
A 28-year-old woman comes to the physician with a history of bright red blood in her stools for 3 days. She has defecated once per day. She does not have fever, pain on defecation, or abdominal pain. She was treated for a urinary tract infection with levofloxacin around 3 months ago. Menses occur at regular intervals of 28–30 days and lasts 3–4 days. Her father died of colon cancer 4 years ago. Her only medication is an iron supplement. She is 162 cm (5 ft 4 in) tall and weighs 101.2 kg (223 lbs); BMI is 38.3 kg/m2. Her temperature is 36.5°C (97.7°F), pulse is 89/min, and blood pressure is 130/80 mm Hg. Rectal examination shows anal skin tags. Anoscopy shows multiple enlarged bluish veins above the dentate line at 7 and 11 o'clock positions. When asked to exhale through a closed nostril a mass prolapses but spontaneously reduces when breathing normally. Which of the following is the most appropriate next step in management?
A 45-year-old woman comes to the office with a 2-week history of rectal bleeding that occurs every day with her bowel movements. She denies any pain during defecation. Apart from this, she does not have any other complaints. Her past medical history is insignificant except for 5 normal vaginal deliveries. Her vitals are a heart rate of 72/min, a respiratory rate of 15/min, a temperature of 36.7°C (98.1°F), and a blood pressure of 115/85 mm Hg. On rectovaginal examination, there is a palpable, non-tender, prolapsed mass that can be pushed back by the examiner's finger into the anal sphincter. What is the most likely diagnosis?
A 34-year-old woman with no significant prior medical history presents to the clinic with several days of bloody stool. She also complains of constipation and straining, but she has no other symptoms. She has no family history of colorectal cancer or inflammatory bowel disease. She does not smoke or drink alcohol. Her vital signs are as follows: blood pressure is 121/81 mm Hg, heart rate is 77/min, and respiratory rate is 15/min. There is no abdominal discomfort on physical exam, and a digital rectal exam reveals bright red blood. Of the following, which is the most likely diagnosis?
A 38-year-old man comes to the physician because of a 2-week history of severe pain while passing stools. The stools are covered with bright red blood. He has been avoiding defecation because of the pain. Last year, he was hospitalized for pilonidal sinus surgery. He has had chronic lower back pain ever since he had an accident at his workplace 10 years ago. The patient's father was diagnosed with colon cancer at the age of 62. Current medications include oxycodone and gabapentin. He is 163 cm (5 ft 4 in) tall and weighs 100 kg (220 lb); BMI is 37.6 kg/m2. Vital signs are within normal limits. The abdomen is soft and nontender. Digital rectal examination was not performed because of severe pain. His hemoglobin is 16.3 mg/dL and his leukocyte count is 8300/mm3. Which of the following is the most appropriate next step in management?
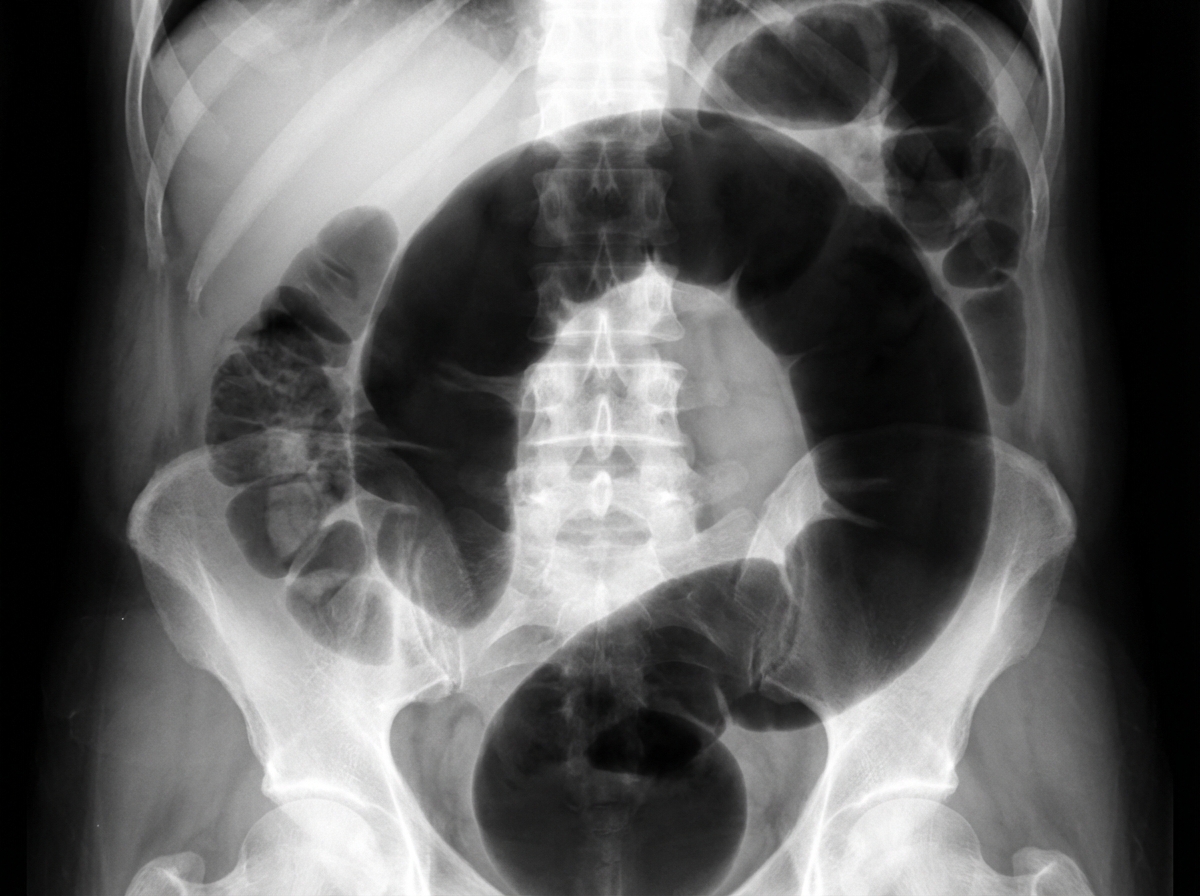
An institutionalized 65-year-old man is brought to the emergency department because of abdominal pain and distension for 12 hours. The pain was acute in onset and is a cramping-type pain associated with nausea, vomiting, and constipation. He has a history of chronic constipation and has used laxatives for years. There is no history of inflammatory bowel disease in his family. He has not been hospitalized recently. There is no recent history of weight loss or change in bowel habits. On physical examination, the patient appears ill. The abdomen is distended with tenderness mainly in the left lower quadrant and is tympanic on percussion. The blood pressure is 110/79 mm Hg, heart rate is 100/min, the respiratory rate is 20/min, and the temperature is 37.2°C (99.0°F). The CBC shows an elevated white blood cell count. The plain abdominal X-ray is shown in the accompanying image. What is the most likely cause of his condition?
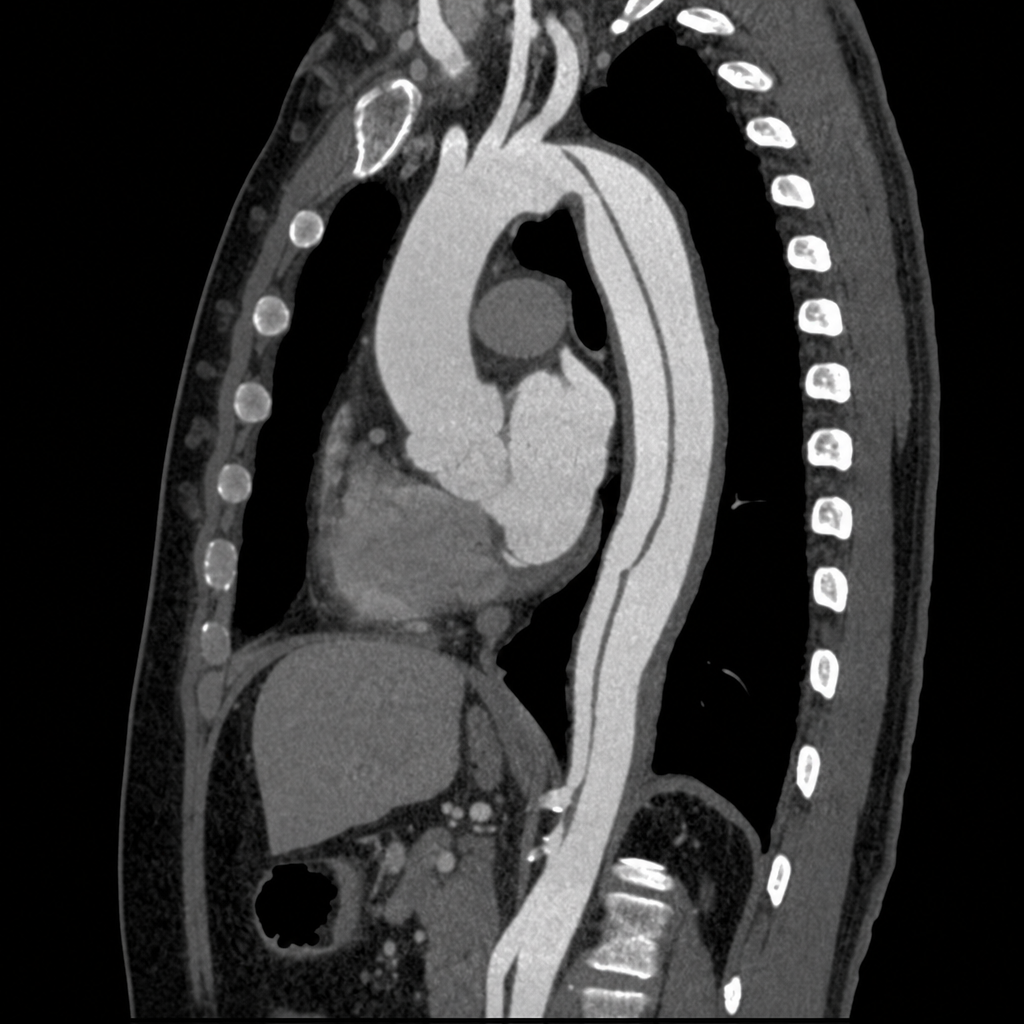
A 55-year-old man presents to the emergency department with sudden-onset tearing chest pain radiating to the interscapular region. He has a history of poorly controlled hypertension. BP is 178/96 mmHg in the right arm and 142/80 mmHg in the left arm. He is diaphoretic and in moderate distress. A CT angiogram of the chest is obtained. The image demonstrates an intimal flap originating 3 cm distal to the left subclavian artery with the false lumen extending through the descending thoracic aorta to the level of the renal arteries; the ascending aorta and aortic root appear normal. Which of the following is the most appropriate management?
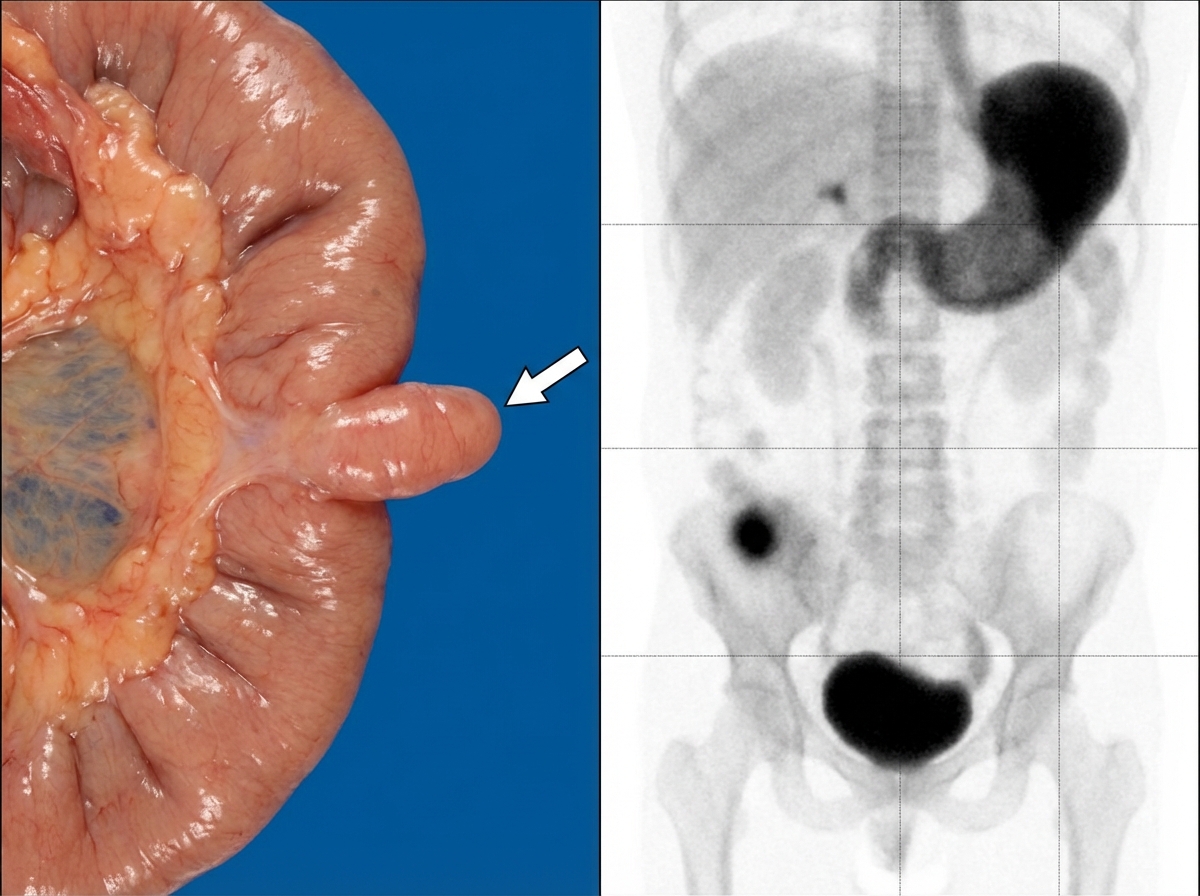
A 67-year-old woman with a history of atrial fibrillation on warfarin presents with sudden-onset severe periumbilical pain out of proportion to physical examination findings. She has a heart rate of 110 bpm, blood pressure of 88/60 mmHg, and temperature of 37.2°C. Her abdomen is rigid with diffuse tenderness, guarding, and rebound on palpation. Serum lactate is 4.8 mmol/L. CT angiography of the abdomen with contrast demonstrates a filling defect at the origin of the superior mesenteric artery consistent with embolus, pneumatosis intestinalis of the small bowel, and portal venous gas. Which of the following is the most appropriate next step in management?

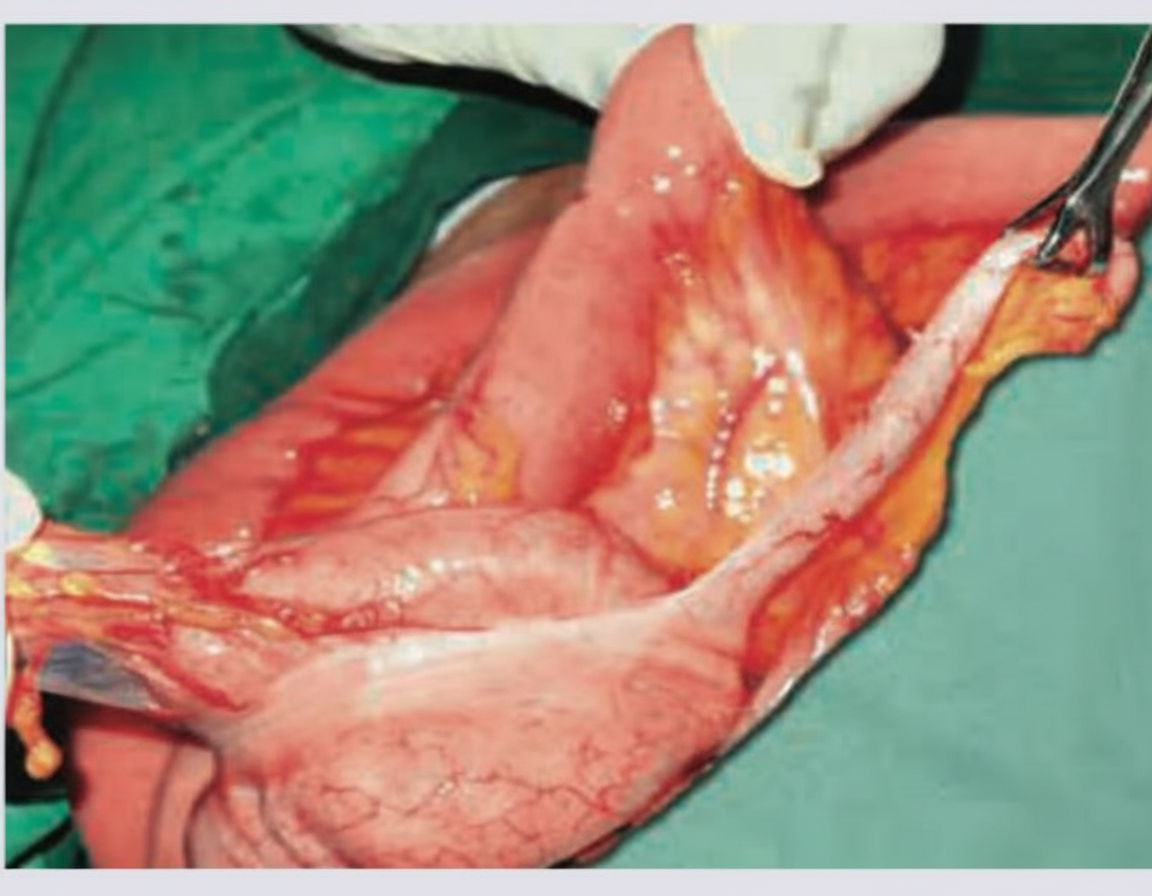
The following image shows \qquad and the test being performed is \qquad ?
All the following statements regarding this condition are true except:
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app