
Gastrointestinal Surgery — MCQs

On this page
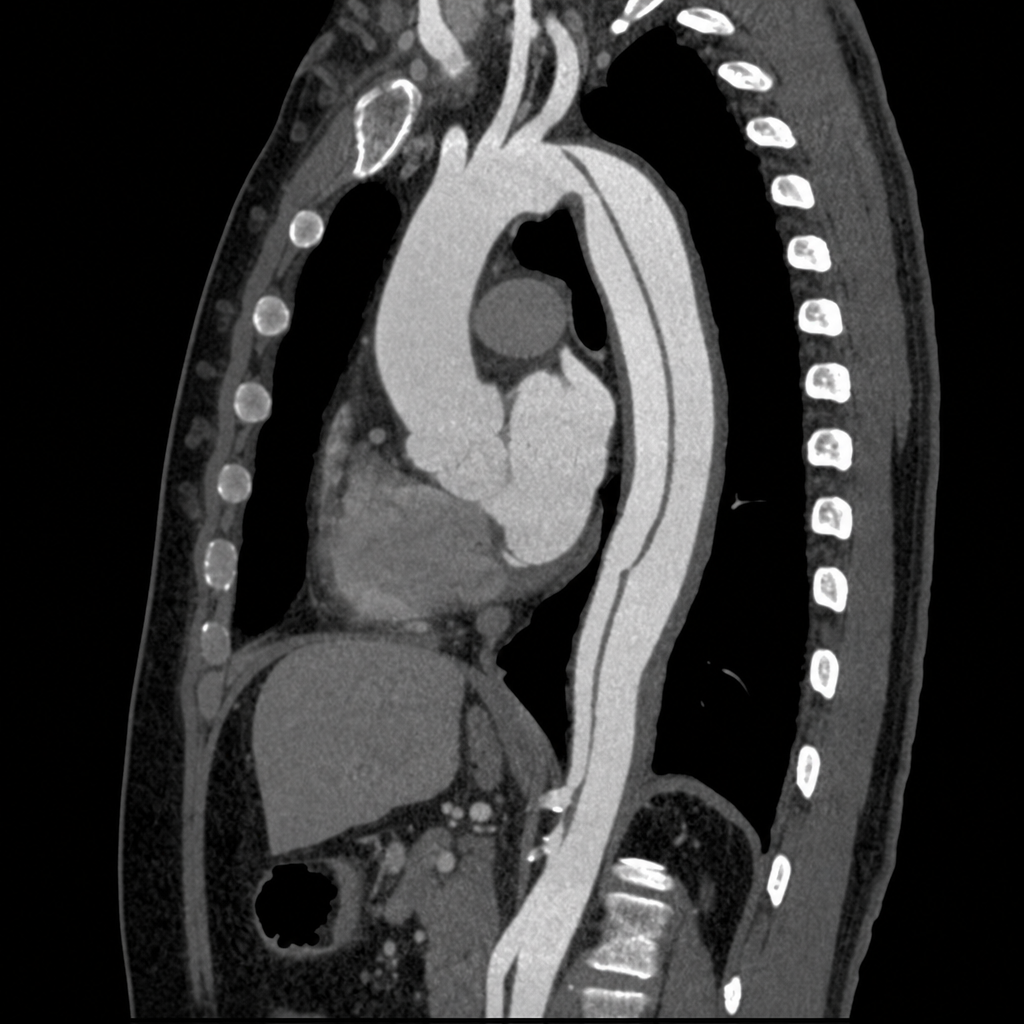
A 55-year-old man presents to the emergency department with sudden-onset tearing chest pain radiating to the interscapular region. He has a history of poorly controlled hypertension. BP is 178/96 mmHg in the right arm and 142/80 mmHg in the left arm. He is diaphoretic and in moderate distress. A CT angiogram of the chest is obtained. The image demonstrates an intimal flap originating 3 cm distal to the left subclavian artery with the false lumen extending through the descending thoracic aorta to the level of the renal arteries; the ascending aorta and aortic root appear normal. Which of the following is the most appropriate management?
A 67-year-old woman with a history of atrial fibrillation on warfarin presents with sudden-onset severe periumbilical pain out of proportion to physical examination findings. She has a heart rate of 110 bpm, blood pressure of 88/60 mmHg, and temperature of 37.2°C. Her abdomen is rigid with diffuse tenderness, guarding, and rebound on palpation. Serum lactate is 4.8 mmol/L. CT angiography of the abdomen with contrast demonstrates a filling defect at the origin of the superior mesenteric artery consistent with embolus, pneumatosis intestinalis of the small bowel, and portal venous gas. Which of the following is the most appropriate next step in management?

The following image shows \qquad and the test being performed is \qquad ?
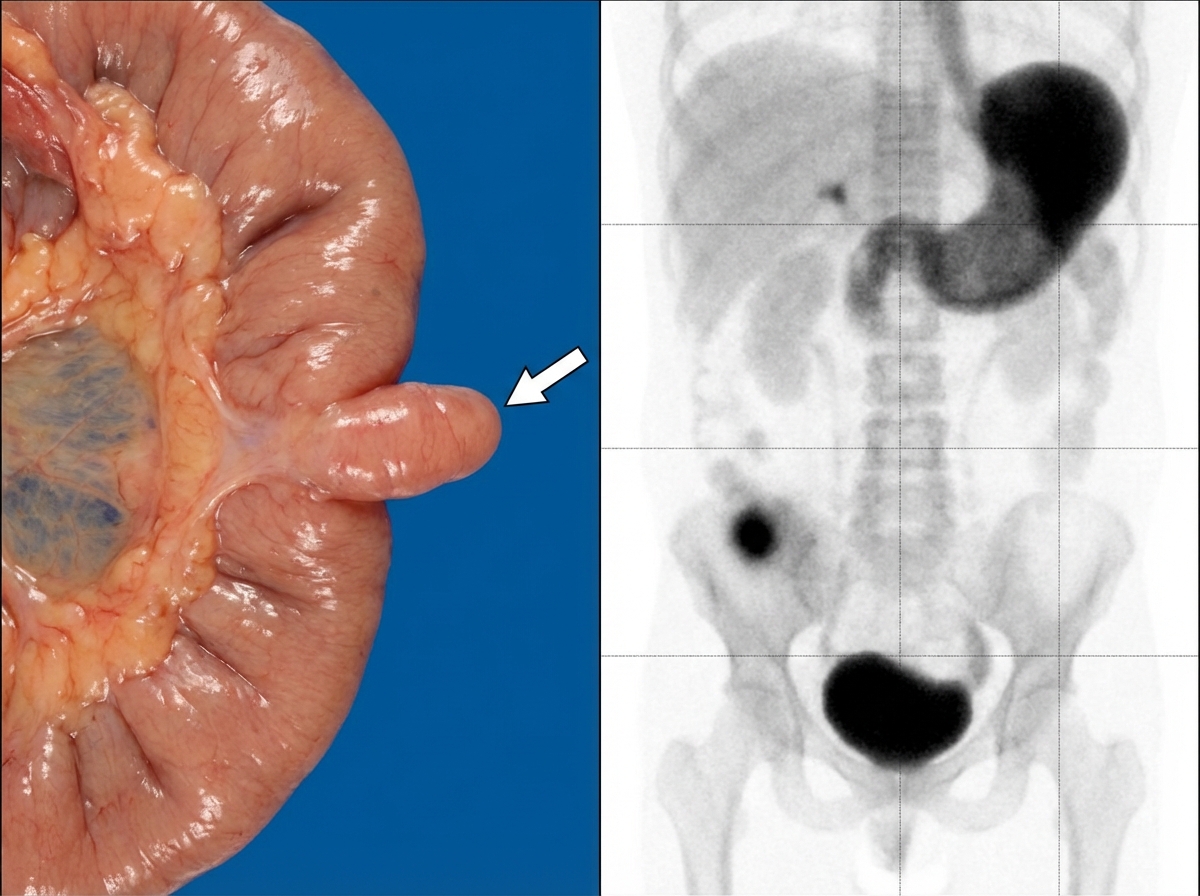
All the following statements regarding this condition are true except:
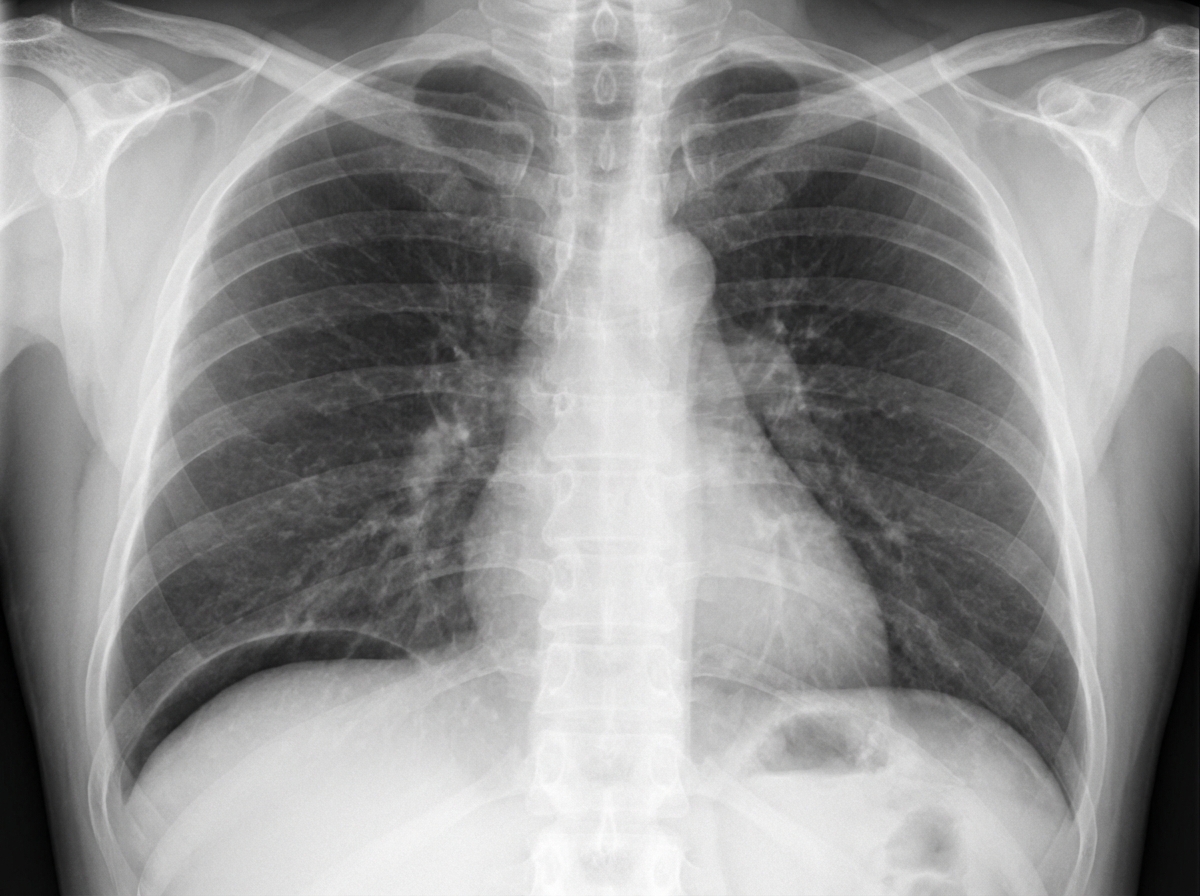
A 34-year-old male patient complains of sudden severe epigastric pain along with vomiting, tenderness, guarding. On examination there is abdominal rigidity and tachycardia. He admits to taking NSAIDs for pain. The radiological examination of the patient is given below. All statements given below are true except?
Identify the tube shown in the image:

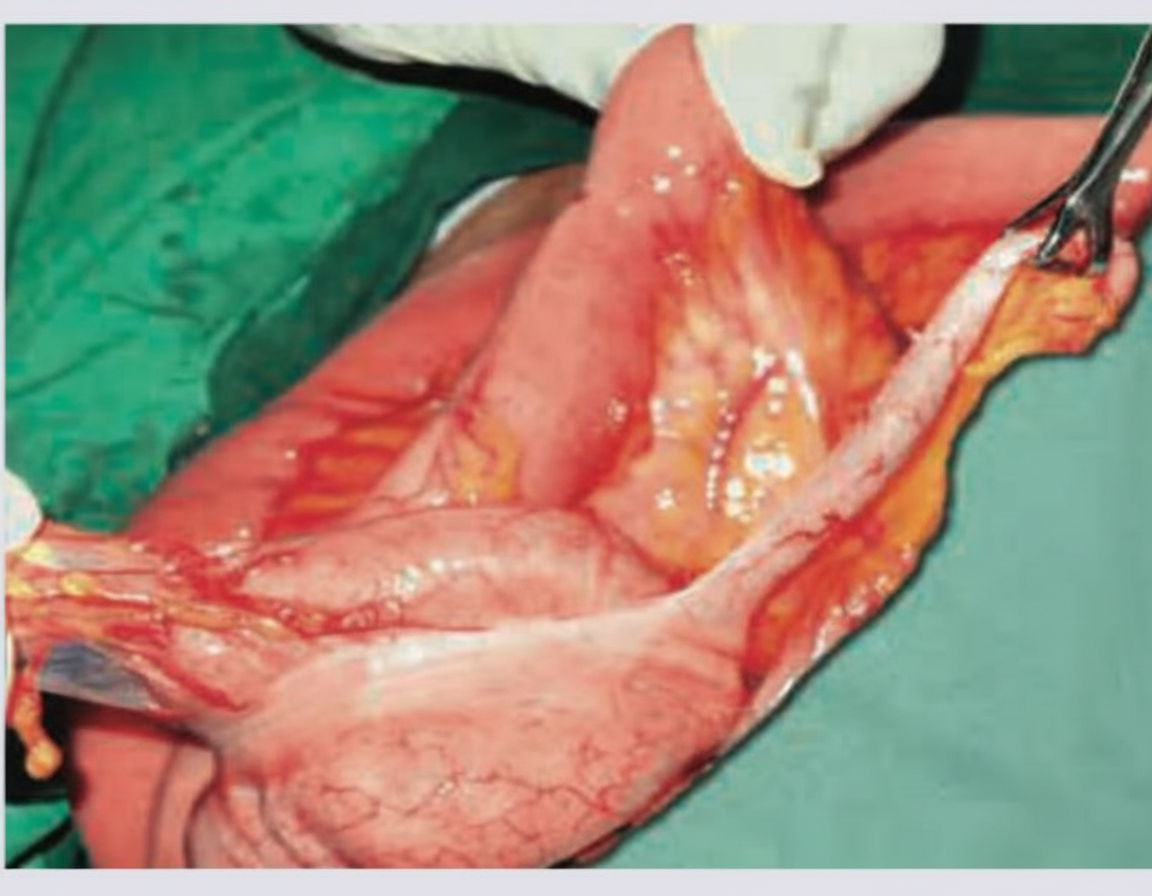
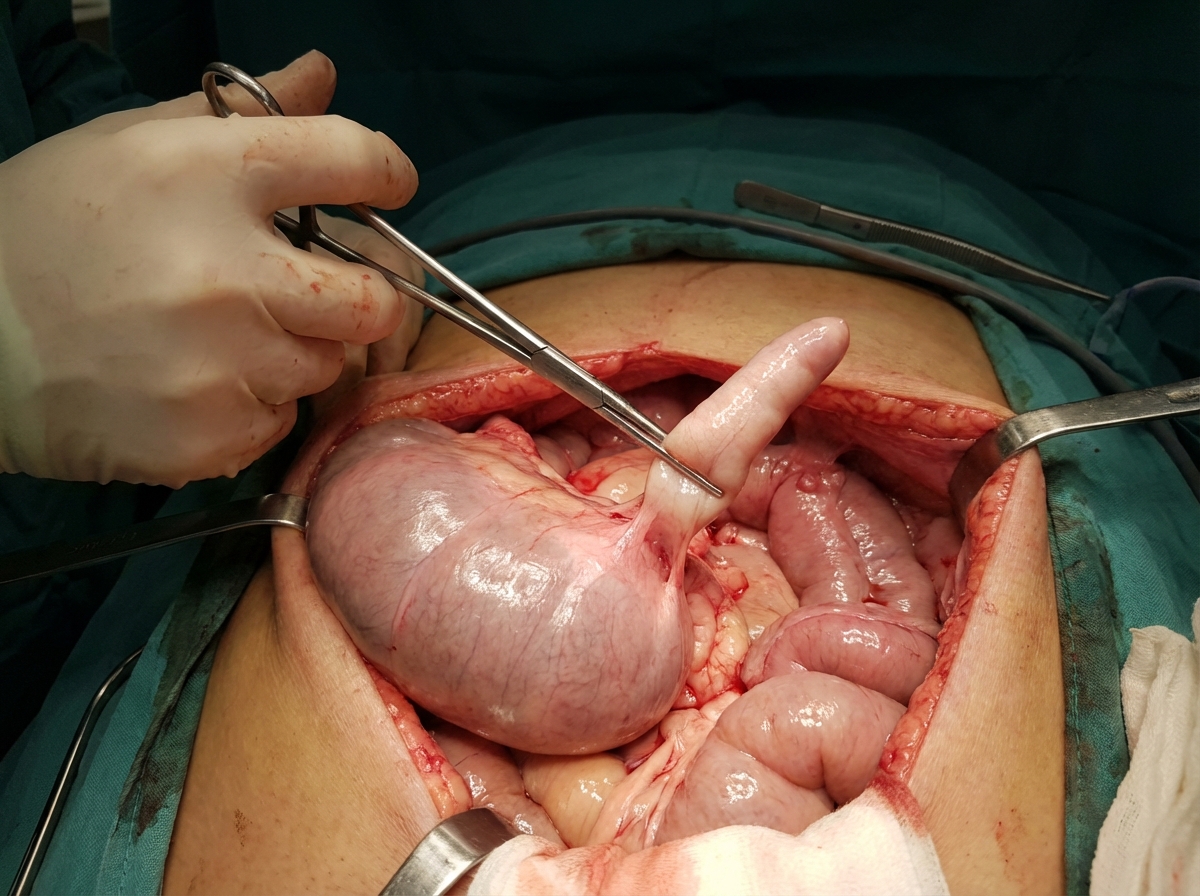
Identify the structure held with artery forceps:
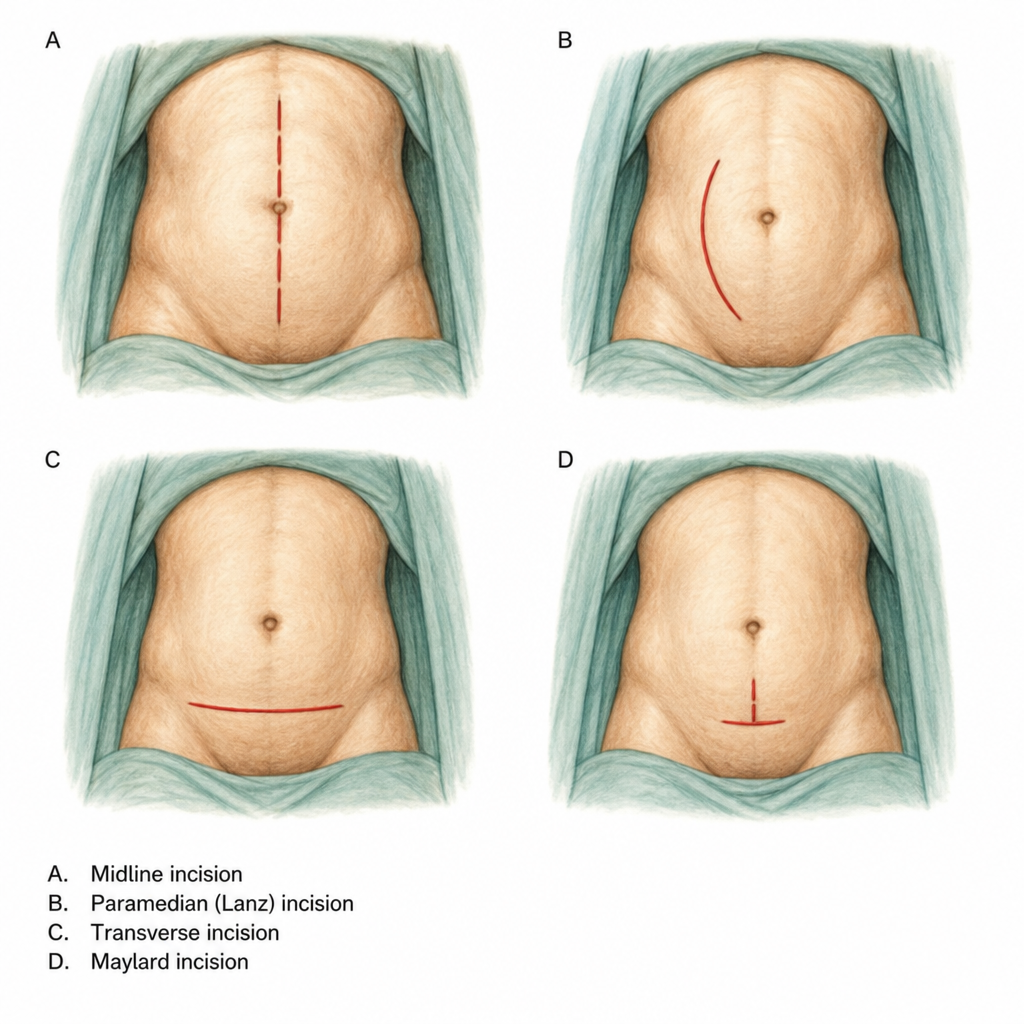
Which of the following is Lanz incision?
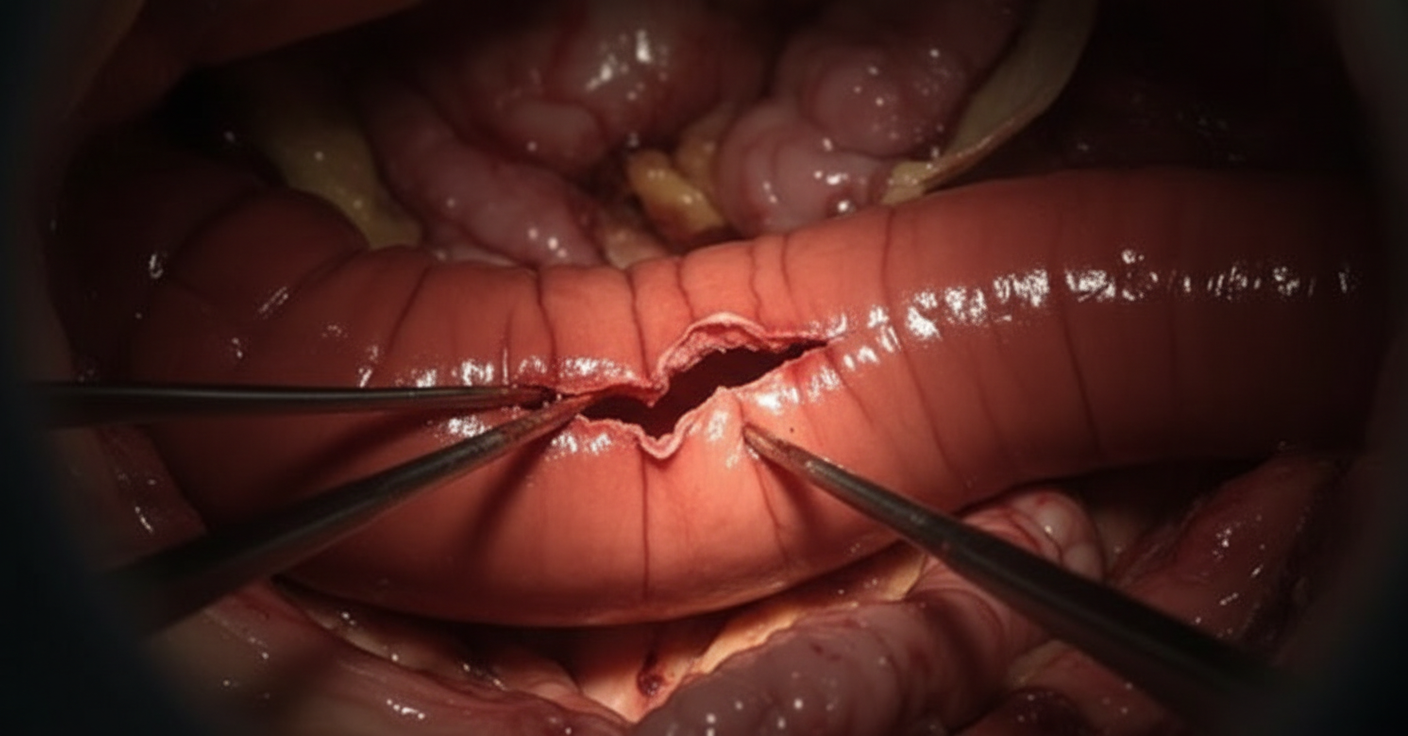
The following is appearance of bowel intraoperatively. Which is correct about the condition?
A 30-year-old man presents with abdominal pain and fever for one day. He has history of diarrhea for last several months which contains blood. What is the diagnosis?

Practice by Chapter
Anorectal procedures
Practice Questions
Bariatric surgery procedures and complications
Practice Questions
Colorectal cancer resection principles
Practice Questions
Elective colorectal procedures
Practice Questions
Esophageal surgery procedures
Practice Questions
Gastric surgery procedures
Practice Questions
Hepatobiliary surgery basics
Practice Questions
Inflammatory bowel disease surgical management
Practice Questions
Liver resection principles
Practice Questions
Ostomy creation and management
Practice Questions
Pancreatic surgery procedures
Practice Questions
Small bowel resection and anastomosis
Practice Questions
Whipple procedure indications
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app