
Breast Surgery — MCQs

On this page
A 45-year-old woman presents with a 2 cm palpable mass in the upper outer quadrant of her right breast. Mammography shows a spiculated lesion with microcalcifications. Core needle biopsy reveals invasive ductal carcinoma, ER-positive, PR-positive, HER2-negative. Sentinel lymph node biopsy shows no metastases. Apply the appropriate surgical management.
Which of the following statements is wrong regarding phyllodes tumor of the breast? (Recent NEET Pattern 2016-17)
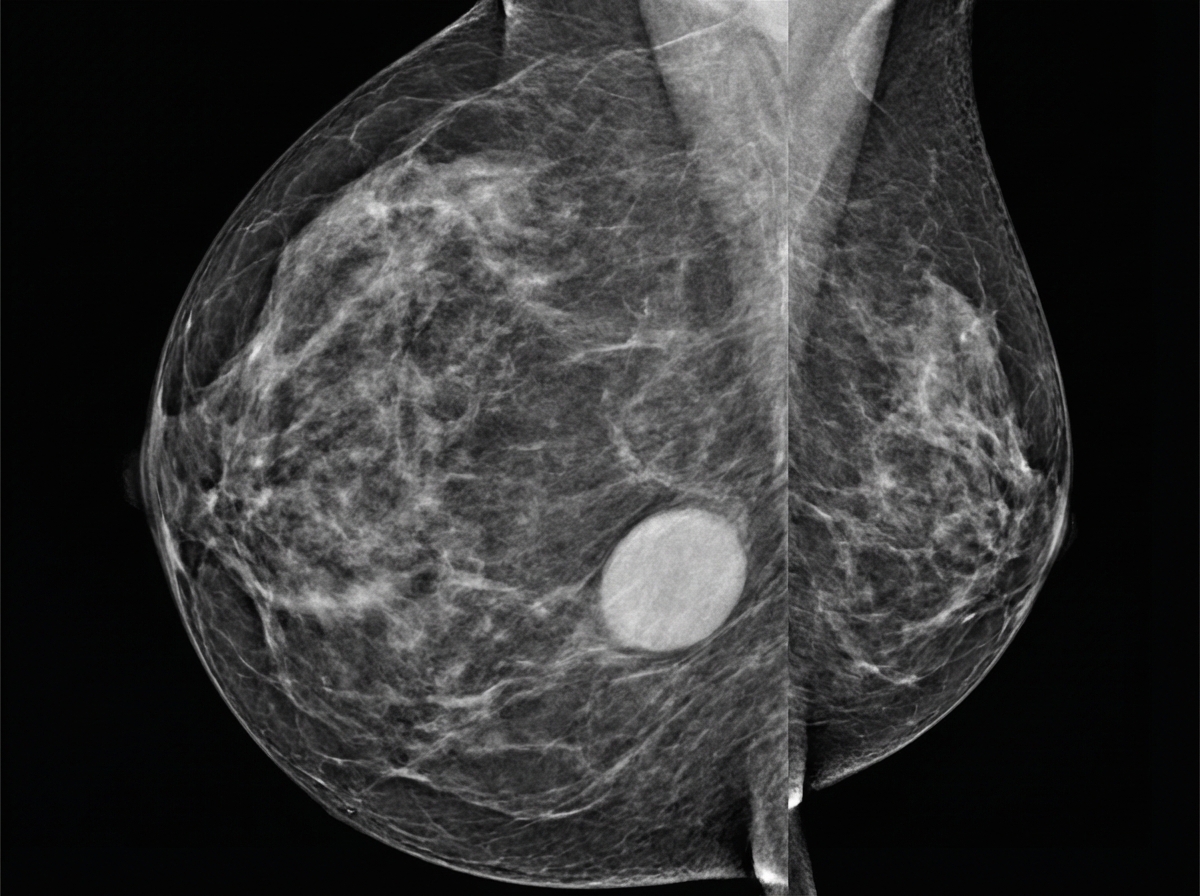
A 24-year-old female patient presents with a right breast mass. On physical examination this breast mass is hyper mobile and soft. The mammogram is shown below. Ultrasound of the right breast demonstrates an oval, circumscribed, parallel, hypoechoic solid mass. What is the most possible diagnosis?
What is the diagnosis of the patient shown in the image? (Recent NEET Pattern 2016-17)

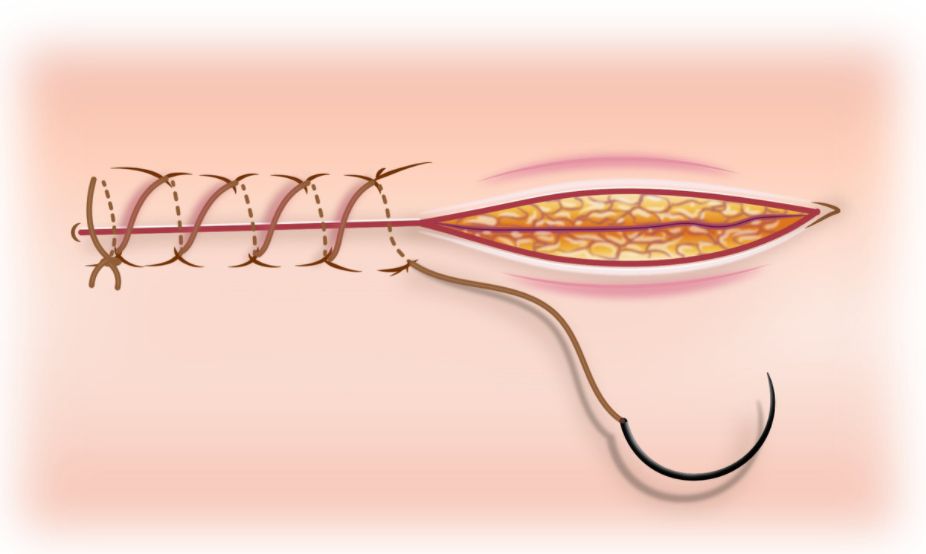
The surgeon attending has completed a modified radical mastectomy for a carcinoma breast patient. You have to suture the wound using subcuticular sutures. Which absorbable monofilament with relatively rapid loss of tensile strength suture would you choose for buried superficial skin closure?
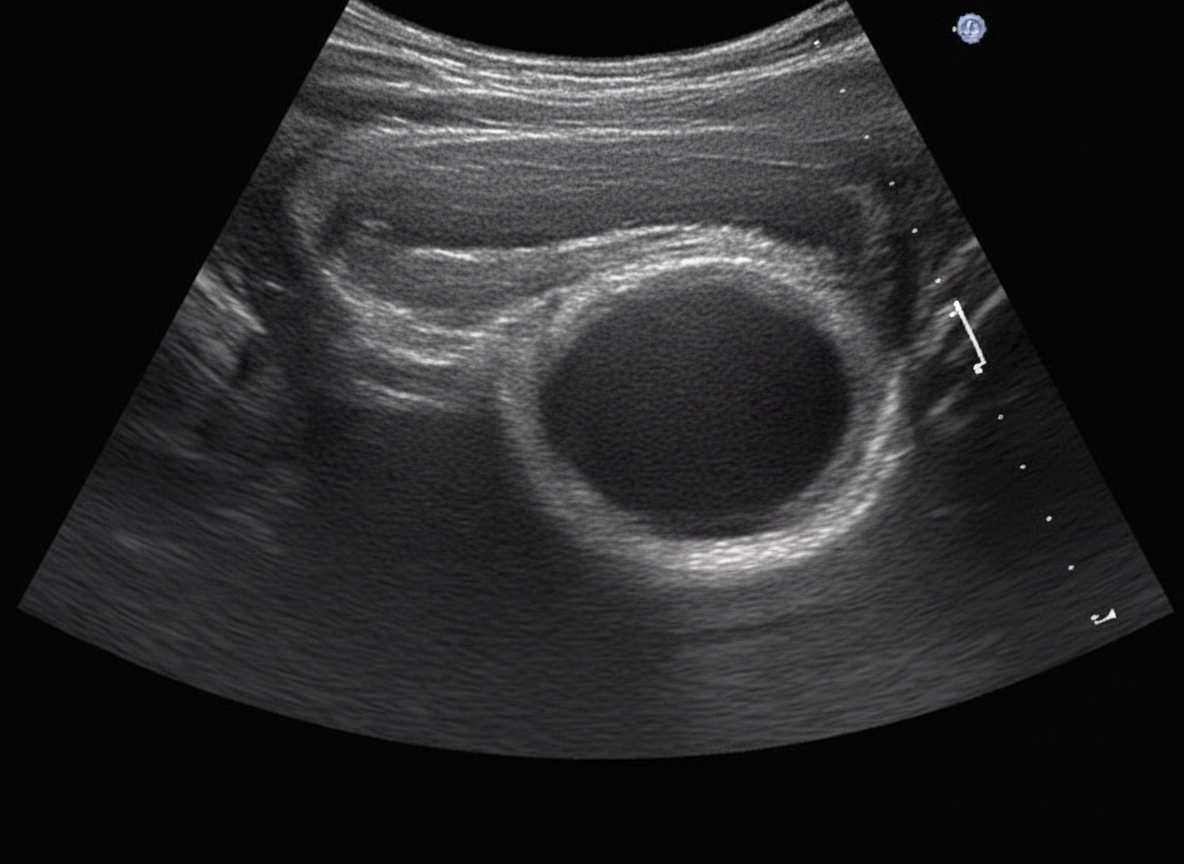
A 28-year-old woman presents with a painless breast lump. Ultrasound shows a solid, oval, circumscribed, hypoechoic mass; core-needle biopsy confirms fibroadenoma. Which of the following is not an objective medical indication for excision in this condition?
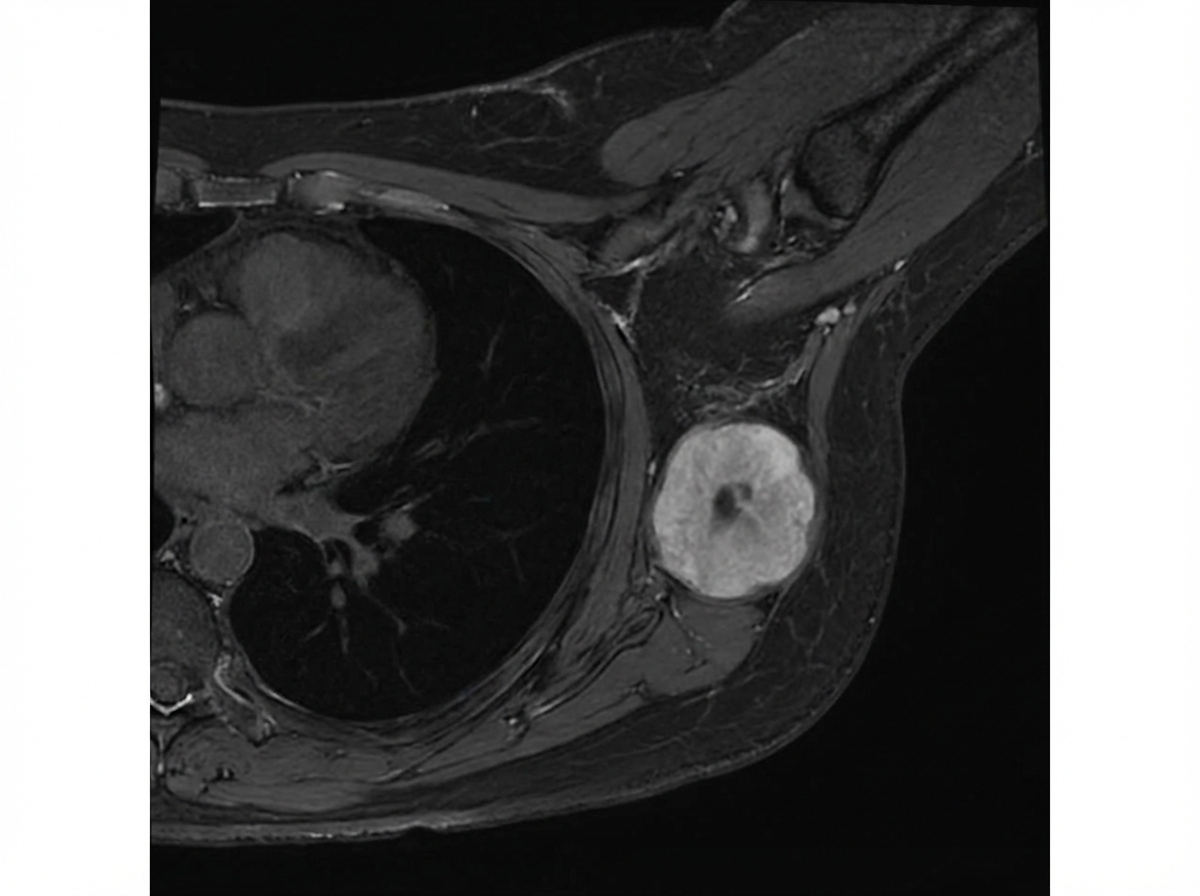
In the MRI breast shown below, a 4 cm mass is present with no nodal metastasis and no distant metastasis. Biopsy confirms invasive breast carcinoma. What is the anatomic stage of this breast cancer?
Practice by Chapter
Axillary lymph node dissection
Practice Questions
Benign breast disease management
Practice Questions
Breast biopsy techniques
Practice Questions
Breast cancer staging and surgical management
Practice Questions
Breast conservation therapy
Practice Questions
Breast reconstruction options
Practice Questions
Hereditary breast cancer syndromes
Practice Questions
Inflammatory breast cancer
Practice Questions
Male breast cancer
Practice Questions
Mastectomy techniques and indications
Practice Questions
Nipple discharge evaluation
Practice Questions
Post-mastectomy complications
Practice Questions
Sentinel lymph node biopsy
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app