
Nipple discharge evaluation — MCQs

A 33-year-old woman presents to her primary care physician for non-bloody nipple discharge. She states that it has been going on for the past month and that it sometimes soils her shirt. The patient drinks 2 to 3 alcoholic beverages per day and smokes 1 pack of cigarettes per day. She is currently seeking mental health treatment with an outpatient psychiatrist after a recent hospitalization for auditory hallucinations. Her psychiatrist prescribed her a medication that she can not recall. Otherwise, she complains of headaches that occur frequently. Her temperature is 98.6°F (37.0°C), blood pressure is 137/68 mmHg, pulse is 70/min, respirations are 13/min, and oxygen saturation is 98% on room air. Physical exam is notable for bilateral galactorrhea that can be expressed with palpation. Which of the following is the best next step in management?
A 37-year-old woman presents to her primary care physician for bilateral nipple discharge. The patient states that she has observed a milky discharge coming from her nipples for the past month. On review of systems, the patient states that she has felt fatigued lately and has experienced decreased libido. She also endorses headaches that typically resolve by the middle of the day and a 5 pound weight gain this past month. The patient has a past medical history of obesity, schizophrenia, and constipation. Her temperature is 99.5°F (37.5°C), blood pressure is 145/95 mmHg, pulse is 60/min, respirations are 15/min, and oxygen saturation is 98% on room air. On physical exam, you note an obese, fatigued-appearing woman. Dermatologic exam reveals fine, thin hair over her body. Cardiopulmonary exam is within normal limits. Neurological exam reveals cranial nerves II-XII as grossly intact. The patient exhibits 1+ sluggish reflexes. Which of the following is the most likely diagnosis?
A 29-year-old nulligravid woman comes to the physician because of a 10-day history of small quantities of intermittent, blood-tinged discharge from her left nipple. There is no personal or family history of serious illness. She has smoked 1 pack of cigarettes daily for 5 years. Her last menstrual period was 12 days ago. She is sexually active and uses condoms inconsistently. Physical examination shows scant serosanguinous fluid expressible from the left nipple. There is no palpable breast mass or axillary lymphadenopathy. Examination shows no other abnormalities. Which of the following is the most appropriate next step in management?
A 36-year-old woman comes to the gynecologist because of a 4-month history of irregular menstrual cycles. Menses occur at irregular 15 to 45-day intervals and last 1–2 days with minimal flow. She also reports a milk-like discharge from her nipples for 3 months, as well as a history of fatigue and muscle and joint pain. She does not have abdominal pain, fever, or headache. She has recently gained 2.5 kg (5.5 lb) of weight. She was diagnosed with schizophrenia and started on aripiprazole by a psychiatrist 8 months ago. She has hypothyroidism but has not been taking levothyroxine for 6 months. She does not smoke or consume alcohol. She appears healthy and anxious. Her vital signs are within normal limits. Pelvic examination shows vaginal atrophy. Visual field and skin examination are normal. Laboratory studies show: Hemoglobin 12.7 g/dL Serum Glucose 88 mg/dL Creatinine 0.7 mg/dL Thyroid-stimulating hormone 16.3 μU/mL Cortisol (8AM) 18 μg/dL Prolactin 88 ng/mL Urinalysis is normal. An x-ray of the chest and ultrasound of the pelvis show no abnormalities. Which of the following is the most likely explanation for the nipple discharge in this patient?
A 47-year-old woman comes to the physician for a mass in her left breast she noticed 2 days ago during breast self-examination. She has hypothyroidism treated with levothyroxine. There is no family history of breast cancer. Examination shows large, moderately ptotic breasts. The mass in her left breast is small (approximately 1 cm x 0.5 cm), firm, mobile, and painless. It is located 4 cm from her nipple-areolar complex at the 7 o'clock position. There are no changes in the skin or nipple, and there is no palpable axillary adenopathy. No masses are palpable in her right breast. A urine pregnancy test is negative. Mammogram showed a soft tissue mass with poorly defined margins. Core needle biopsy confirms a low-grade infiltrating ductal carcinoma. The pathological specimen is positive for estrogen receptors and negative for progesterone and human epidermal growth factor receptor 2 (HER2) receptors. Staging shows no distant metastatic disease. Which of the following is the most appropriate next step in management?
A 50-year-old obese woman presents for a follow-up appointment regarding microcalcifications found in her left breast on a recent screening mammogram. The patient denies any recent associated symptoms. The past medical history is significant for polycystic ovarian syndrome (PCOS), for which she takes metformin. Her menarche occurred at age 11, and the patient still has regular menstrual cycles. The family history is significant for breast cancer in her mother at the age of 72. The review of systems is notable for a 6.8 kg (15 lb) weight loss in the past 2 months. The vital signs include: temperature 37.0°C (98.6°F), blood pressure 130/70 mm Hg, pulse 82/min, respiratory rate 17/min, and oxygen saturation 98% on room air. On physical examination, the patient is alert and cooperative. The breast examination reveals no palpable masses, lymphadenopathy, or evidence of skin retraction. A biopsy of the left breast is performed, and histologic examination demonstrates evidence of non-invasive malignancy. Which of the following is the most appropriate definitive treatment for this patient?
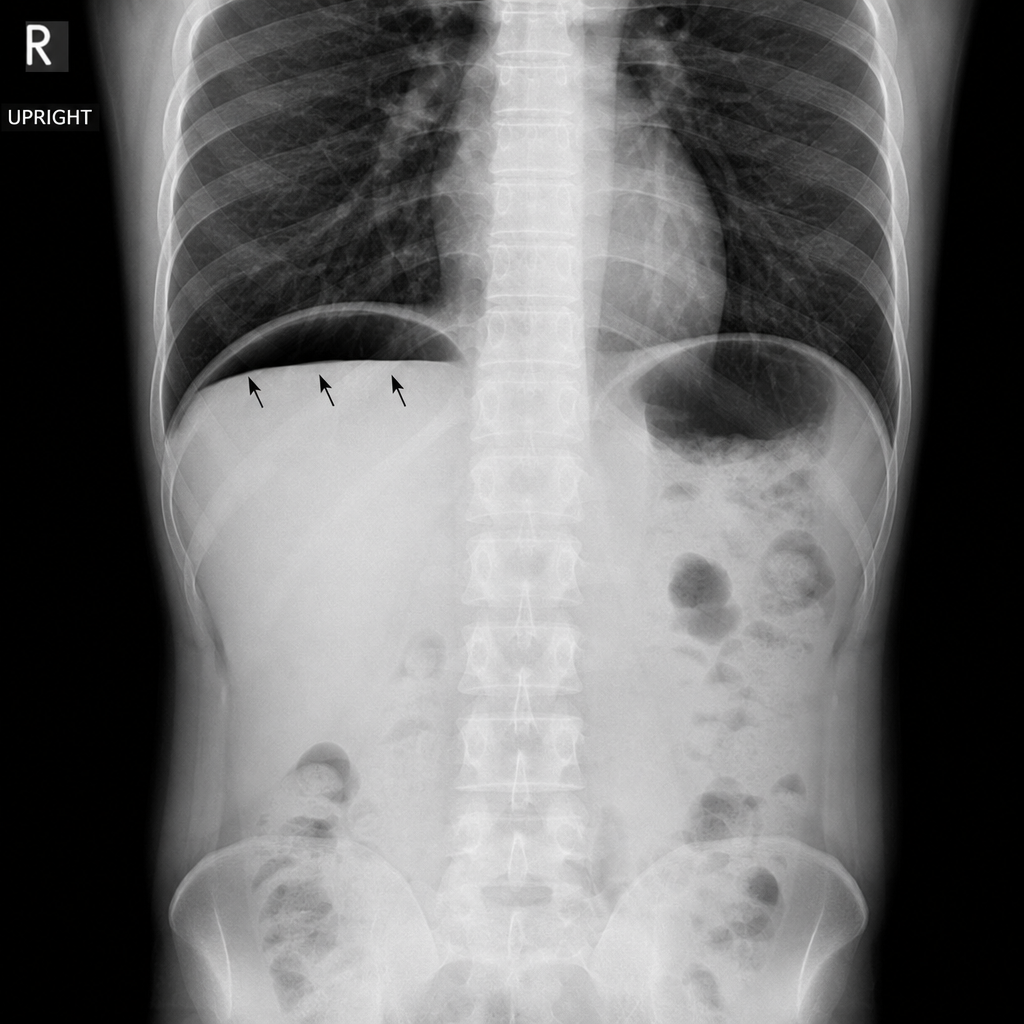
A 45-year-old man presents to the emergency department with a 12-hour history of severe periumbilical pain that has migrated to the right lower quadrant, fever of 38.4°C, and anorexia. On examination, there is point tenderness 2/3 of the way along a line from the umbilicus to the right anterior superior iliac spine. His WBC is 14,200/mm³ with a left shift. A plain abdominal radiograph is obtained. Which of the following findings on this image would most directly indicate perforation requiring urgent surgical intervention?
A 58-year-old woman underwent mastectomy for multicentric DCIS. Final pathology shows high-grade DCIS with comedonecrosis, margins negative by 3 mm, no invasion identified in 40 tissue blocks examined. Sentinel lymph node biopsy shows isolated tumor cells (0.1 mm cluster) positive for cytokeratin. The medical oncologist requests input on systemic therapy. Evaluate the significance of the nodal finding and recommendations.
A 36-year-old woman with BRCA2 mutation and strong family history of breast and ovarian cancer desires risk-reducing surgery. She has 2 young children and plans to have one more child in 2 years. She asks about timing of risk-reducing mastectomy and oophorectomy. Her mother died of ovarian cancer at age 45, and sister diagnosed with breast cancer at age 38. Evaluate the optimal counseling regarding surgical timing.
A 42-year-old premenopausal woman with newly diagnosed 2.5 cm triple-negative breast cancer and 3 positive axillary lymph nodes completed neoadjuvant chemotherapy. Post-treatment MRI shows residual 1 cm mass in breast and 1 abnormal lymph node. She desires breast conservation. The tumor board must evaluate the surgical plan considering residual disease burden and emerging data on post-neoadjuvant therapy.
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app