
Breast Surgery — MCQs

On this page
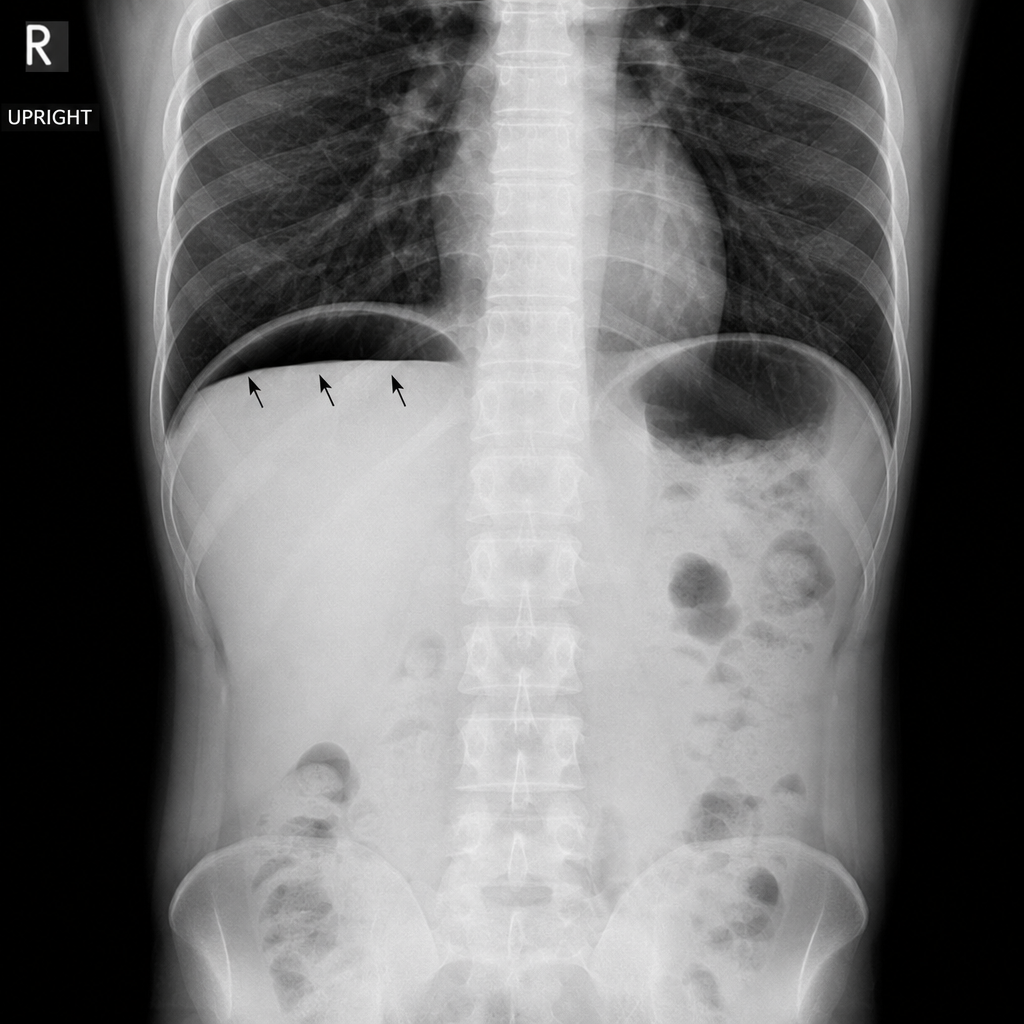
A 45-year-old man presents to the emergency department with a 12-hour history of severe periumbilical pain that has migrated to the right lower quadrant, fever of 38.4°C, and anorexia. On examination, there is point tenderness 2/3 of the way along a line from the umbilicus to the right anterior superior iliac spine. His WBC is 14,200/mm³ with a left shift. A plain abdominal radiograph is obtained. Which of the following findings on this image would most directly indicate perforation requiring urgent surgical intervention?
A 58-year-old woman underwent mastectomy for multicentric DCIS. Final pathology shows high-grade DCIS with comedonecrosis, margins negative by 3 mm, no invasion identified in 40 tissue blocks examined. Sentinel lymph node biopsy shows isolated tumor cells (0.1 mm cluster) positive for cytokeratin. The medical oncologist requests input on systemic therapy. Evaluate the significance of the nodal finding and recommendations.
A 36-year-old woman with BRCA2 mutation and strong family history of breast and ovarian cancer desires risk-reducing surgery. She has 2 young children and plans to have one more child in 2 years. She asks about timing of risk-reducing mastectomy and oophorectomy. Her mother died of ovarian cancer at age 45, and sister diagnosed with breast cancer at age 38. Evaluate the optimal counseling regarding surgical timing.
A 42-year-old premenopausal woman with newly diagnosed 2.5 cm triple-negative breast cancer and 3 positive axillary lymph nodes completed neoadjuvant chemotherapy. Post-treatment MRI shows residual 1 cm mass in breast and 1 abnormal lymph node. She desires breast conservation. The tumor board must evaluate the surgical plan considering residual disease burden and emerging data on post-neoadjuvant therapy.
A 70-year-old woman with multiple comorbidities (COPD, CHF, DM) presents with a 3 cm palpable breast mass. Core biopsy shows invasive ductal carcinoma, ER-positive (95%), PR-positive (90%), HER2-negative, grade 1, Ki-67 5%. Staging shows no metastases. Her surgical risk is assessed as high (ASA class 4). Analyze the optimal treatment approach.
Practice by Chapter
Axillary lymph node dissection
Practice Questions
Benign breast disease management
Practice Questions
Breast biopsy techniques
Practice Questions
Breast cancer staging and surgical management
Practice Questions
Breast conservation therapy
Practice Questions
Breast reconstruction options
Practice Questions
Hereditary breast cancer syndromes
Practice Questions
Inflammatory breast cancer
Practice Questions
Male breast cancer
Practice Questions
Mastectomy techniques and indications
Practice Questions
Nipple discharge evaluation
Practice Questions
Post-mastectomy complications
Practice Questions
Sentinel lymph node biopsy
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app