
ATLS protocols — MCQs

On this page
A 17-year-old male is brought to the emergency department following a motor vehicle accident. He has suffered several wounds and is minimally responsive. There is a large laceration on his forehead as well as a fracture of his nasal bridge. He appears to be coughing and spitting blood. He is already wearing a soft collar. Vitals are as follows: T 36.4C, BP 102/70 mmHg, HR 126 bpm, RR 18/min, and SpO2 is 88% on RA. He has 2 peripheral IVs and received 2L of IV normal saline on route to the hospital. There is frank blood in the oropharynx. Breath sounds are present bilaterally. Abdomen is distended and tender. Pulses are 1+. Which of the following should be the first step in management?
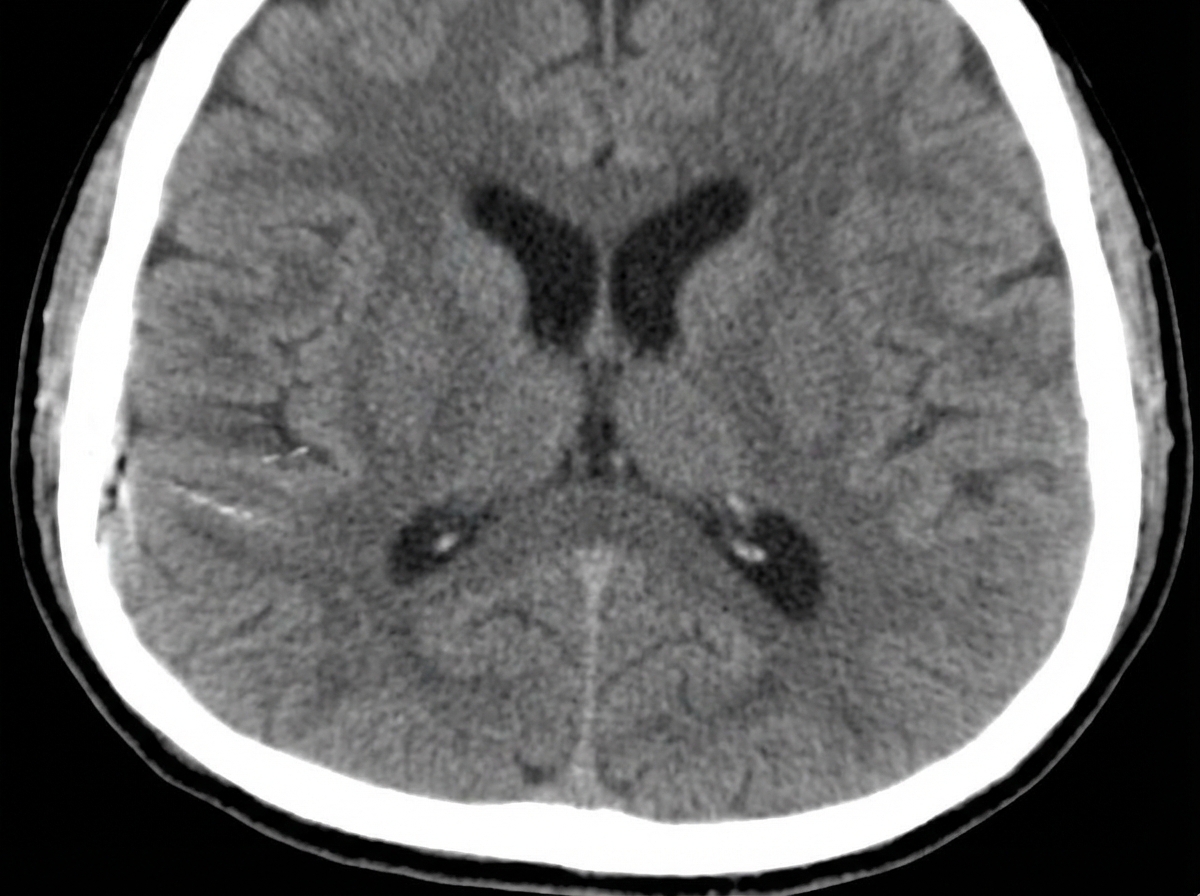
A 31-year-old unresponsive man is admitted to the emergency department after a single-vehicle roll-over accident. On primary assessment by paramedics, he was unresponsive. On admission, he opened his eyes to painful stimuli, was not responsive to verbal commands, and demonstrated abnormal flexion of his arms with extension of his legs in response to pain. The patient was intubated and examined. The blood pressure is 150/90 mm Hg; the heart rate, 56/min; the respiratory rate, 14/min (ventilator-assisted); the temperature, 37.5℃ (99.5℉), and the SpO2, 98% on FiO2 0.40 via mechanical ventilation. The examination shows a depressed fracture of the left temporal bone and ecchymoses and scratches over his abdomen and extremities. His pupils are round, equal, and show a poor response to light. There is no disconjugate eye deviation. His lungs are clear to auscultation and the heart sounds are normal. Abdominal examination reveals normal bowel sounds and no fluid wave. There are no meningeal signs. Focused assessment with sonography for trauma is negative for blood in the abdominal cavity. Head CT scan is shown in the picture. Which procedure is required to guide further management?
A 19-year-old man is rushed to the emergency department 30 minutes after diving head-first into a shallow pool of water from a cliff. He was placed on a spinal board and a rigid cervical collar was applied by the emergency medical technicians. On arrival, he is unconscious and withdraws all extremities to pain. His temperature is 36.7°C (98.1°F), pulse is 70/min, respirations are 8/min, and blood pressure is 102/70 mm Hg. Pulse oximetry on room air shows an oxygen saturation of 96%. The pupils are equal and react sluggishly to light. There is a 3-cm (1.2-in) laceration over the forehead. The lungs are clear to auscultation. Cardiac examination shows no abnormalities. The abdomen is soft and nontender. There is a step-off palpated over the cervical spine. Which of the following is the most appropriate next step in management?
A 45-year-old female presents to the emergency room as a trauma after a motor vehicle accident. The patient was a restrained passenger who collided with a drunk driver traveling approximately 45 mph. Upon impact, the passenger was able to extricate herself from the crushed car and was sitting on the ground at the scene of the accident. Her vitals are all stable. On physical exam, she is alert and oriented, speaking in complete sentences with a GCS of 15. She has a cervical spine collar in place and endorses exquisite cervical spine tenderness on palpation. Aside from her superficial abrasions on her right lower extremity, the rest of her examination including FAST exam is normal. Rapid hemoglobin testing is within normal limits. What is the next best step in management of this trauma patient?
A 45-year-old man was a driver in a motor vehicle collision. The patient is not able to offer a medical history during initial presentation. His temperature is 97.6°F (36.4°C), blood pressure is 104/74 mmHg, pulse is 150/min, respirations are 12/min, and oxygen saturation is 98% on room air. On exam, he does not open his eyes, he withdraws to pain, and he makes incomprehensible sounds. He has obvious signs of trauma to the chest and abdomen. His abdomen is distended and markedly tender to palpation. He also has an obvious open deformity of the left femur. What is the best initial step in management?
Practice by Chapter
Primary survey (ABCDE)
Practice Questions
Airway management in trauma
Practice Questions
Breathing assessment and management
Practice Questions
Circulation assessment and hemorrhage control
Practice Questions
Disability assessment (neurological status)
Practice Questions
Exposure and environmental control
Practice Questions
Secondary survey principles
Practice Questions
Trauma imaging principles
Practice Questions
Trauma team organization
Practice Questions
Mass casualty triage
Practice Questions
Trauma in special populations (pediatric, geriatric)
Practice Questions
Trauma scoring systems
Practice Questions
Trauma quality improvement
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app