
Airway management in trauma — MCQs

A 52-year-old obese man is brought to the emergency department 30 minutes after he was involved in a high-speed motor vehicle collision. He was the unrestrained driver. On arrival, he is lethargic. His pulse is 112/min, respirations are 10/min and irregular, and blood pressure is 94/60 mm Hg. Pulse oximetry on room air shows an oxygen saturation of 91%. The pupils are equal and react sluggishly to light. He withdraws his extremities to pain. There are multiple bruises over his face, chest, and abdomen. Breath sounds are decreased over the left lung base. Two large bore peripheral venous catheters are inserted and 0.9% saline infusion is begun. Rapid sequence intubation is initiated and endotracheal intubation is attempted without success. Bag and mask ventilation is continued. Pulse oximetry shows an oxygen saturation of 84%. The patient has no advance directive and family members have not arrived. Which of the following is the most appropriate next step in the management of this patient?
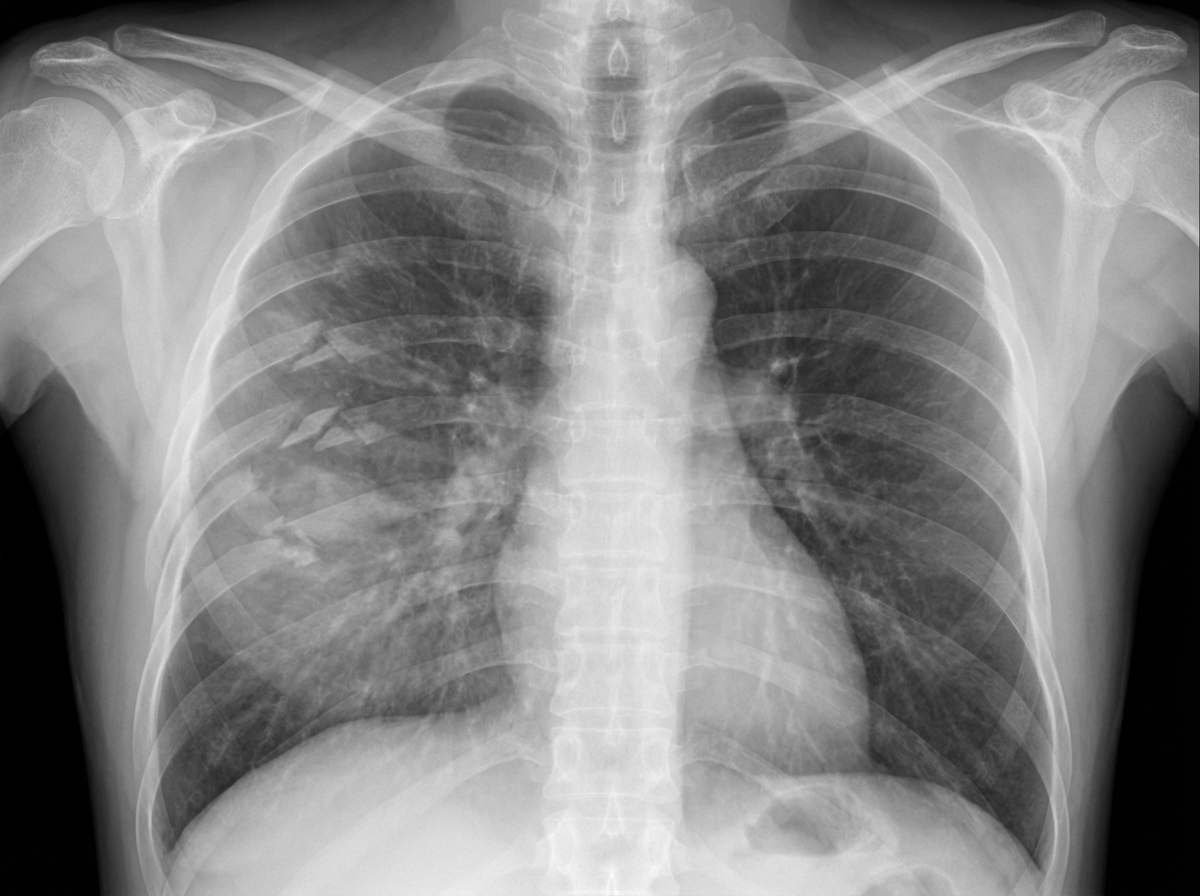
A 27-year-old man is brought to the emergency department 45 minutes after being involved in a motor vehicle collision. He is agitated. He has pain in his upper right arm, which he is cradling in his left arm. His temperature is 36.7°C (98°F), pulse is 135/min, respirations are 25/min, and blood pressure is 145/90 mm Hg. His breathing is shallow. Pulse oximetry on 100% oxygen via a non-rebreather face mask shows an oxygen saturation of 83%. He is confused and oriented only to person. Examination shows multiple bruises on the right anterior thoracic wall. The pupils are equal and reactive to light. On inspiration, his right chest wall demonstrates paradoxical inward movement while his left chest wall is expanding. There is pain to palpation and crepitus over his right anterior ribs. The remainder of the examination shows no abnormalities. An x-ray of the chest is shown. Two large-bore IVs are placed. After fluid resuscitation and analgesia, which of the following is the most appropriate next step in management?
A 21-year-old woman comes to the physician for the evaluation of dry cough and some chest tightness for the past several weeks. The cough is worse at night and while playing volleyball. She frequently has a runny nose and nasal congestion. Her mother has systemic lupus erythematosus. The patient has smoked one pack of cigarettes daily for the last 5 years. She does not drink alcohol. Her only medication is cetirizine. Her vital signs are within normal limits. Pulse oximetry on room air shows an oxygen saturation of 98%. The remainder of the examination shows no abnormalities. Which of the following is the most appropriate next step in management?
A 19-year-old man is rushed to the emergency department 30 minutes after diving head-first into a shallow pool of water from a cliff. He was placed on a spinal board and a rigid cervical collar was applied by the emergency medical technicians. On arrival, he is unconscious and withdraws all extremities to pain. His temperature is 36.7°C (98.1°F), pulse is 70/min, respirations are 8/min, and blood pressure is 102/70 mm Hg. Pulse oximetry on room air shows an oxygen saturation of 96%. The pupils are equal and react sluggishly to light. There is a 3-cm (1.2-in) laceration over the forehead. The lungs are clear to auscultation. Cardiac examination shows no abnormalities. The abdomen is soft and nontender. There is a step-off palpated over the cervical spine. Which of the following is the most appropriate next step in management?
A 28-year-old soldier is brought back to a military treatment facility 45 minutes after sustaining injuries in a building fire from a mortar attack. He was trapped inside the building for around 20 minutes. On arrival, he is confused and appears uncomfortable. He has a Glasgow Coma Score of 13. His pulse is 113/min, respirations are 18/min, and blood pressure is 108/70 mm Hg. Pulse oximetry on room air shows an oxygen saturation of 96%. Examination shows multiple second-degree burns over the chest and bilateral upper extremities and third-degree burns over the face. There are black sediments seen within the nose and mouth. The lungs are clear to auscultation. Cardiac examination shows no abnormalities. The abdomen is soft and nontender. Intravenous fluid resuscitation is begun. Which of the following is the most appropriate next step in management?
A 24-year-old man is brought to the emergency department 30 minutes after being involved in a high-speed motor vehicle collision in which he was a restrained driver. On arrival, he is alert and oriented. His pulse is 112/min, respirations are 29/min, and blood pressure is 100/60 mm Hg. The pupils are equal and reactive to light. There is a 3-cm laceration over the forehead and multiple bruises over the trunk. The lungs are clear to auscultation. Cardiac examination shows no abnormalities. The abdomen is soft and nontender. The right knee is swollen and tender; range of motion is limited by pain. Infusion of 0.9% saline is begun and intravenous acetaminophen is administered. Two hours later, blood-tinged fluid spontaneously drains from both nostrils, and is made worse by leaning forward. On a piece of gauze, it shows up as a rapidly-expanding clear ring of fluid surrounding blood. Further evaluation of this patient is most likely to show which of the following?
An obese 52-year-old man is brought to the emergency department because of increasing shortness of breath for the past 8 hours. Two months ago, he noticed a mass on the right side of his neck and was diagnosed with laryngeal cancer. He has smoked two packs of cigarettes daily for 27 years. He drinks two pints of rum daily. He appears ill. He is oriented to person, place, and time. His temperature is 37°C (98.6°F), pulse is 111/min, respirations are 34/min, and blood pressure is 140/90 mm Hg. Pulse oximetry on room air shows an oxygen saturation of 89%. Examination shows a 9-cm, tender, firm subglottic mass on the right side of the neck. Cervical lymphadenopathy is present. His breathing is labored and he has audible inspiratory stridor but is able to answer questions. The lungs are clear to auscultation. Arterial blood gas analysis on room air shows: pH 7.36 PCO2 45 mm Hg PO2 74 mm Hg HCO3- 25 mEq/L He has no advanced directive. Which of the following is the most appropriate next step in management?
A 17-year-old boy is brought to the emergency department by his brother after losing consciousness 1 hour ago. The brother reports that the patient was skateboarding outside when he fell on the ground and started to have generalized contractions. There was also some blood coming from his mouth. The contractions stopped after about 1 minute, but he remained unconscious for a few minutes afterward. He has never had a similar episode before. There is no personal or family history of serious illness. He does not smoke or drink alcohol. He does not use illicit drugs. He takes no medications. On arrival, he is confused and oriented only to person and place. He cannot recall what happened and reports diffuse muscle ache, headache, and fatigue. He appears pale. His temperature is 37°C (98.6°F), pulse is 80/min, and blood pressure is 130/80 mm Hg. There is a small wound on the left side of the tongue. A complete blood count and serum concentrations of electrolytes, urea nitrogen, and creatinine are within the reference ranges. Toxicology screening is negative. An ECG shows no abnormalities. Which of the following is the most appropriate next step in management?
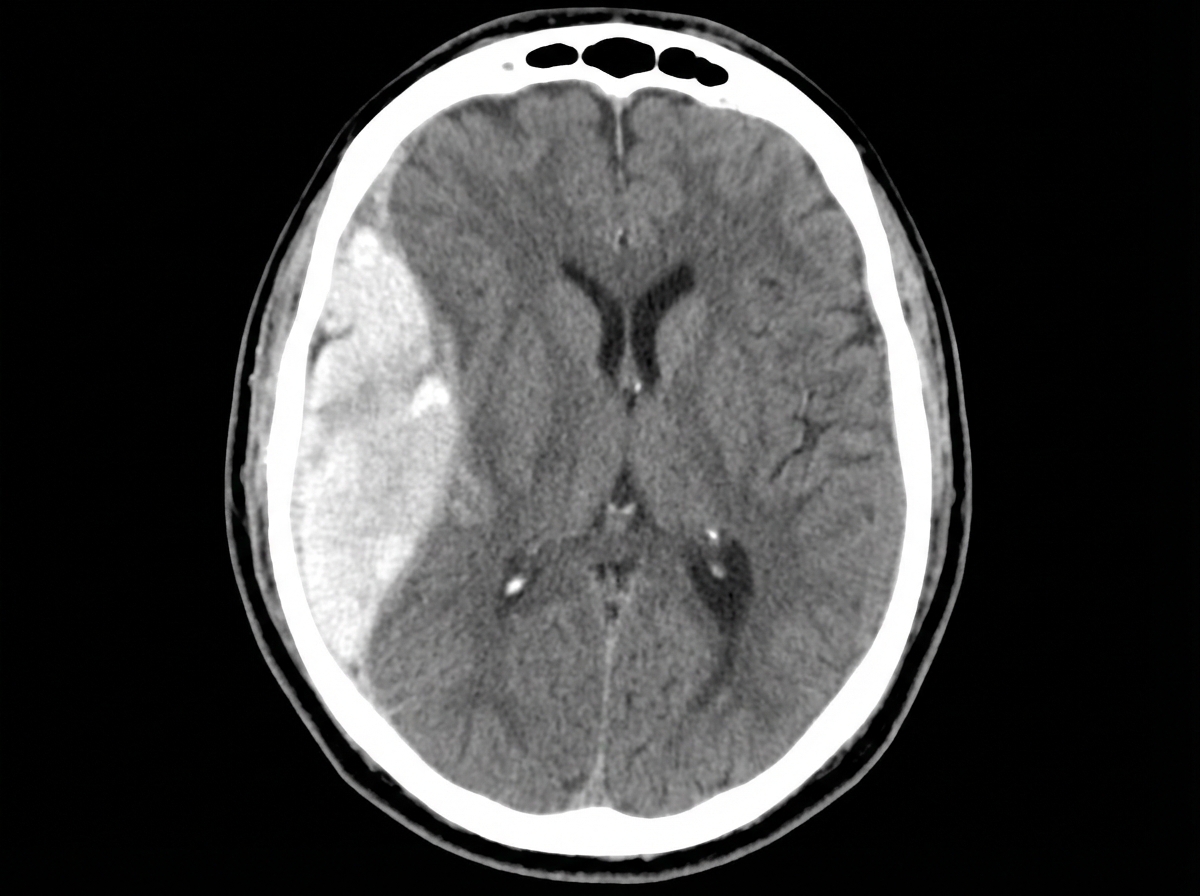
A 47-year-old man is admitted to the emergency room after a fight in which he was hit in the head with a hammer. The witnesses say that the patient initially lost consciousness, but regained consciousness by the time emergency services arrived. On admission, the patient complained of a diffuse headache. He opened his eyes spontaneously, was verbally responsive, albeit confused, and was able to follow commands. He could not elevate his left hand and leg. He did not remember the events prior to the loss of consciousness and had difficulty remembering information, such as the names of nurses or doctors. His airway was not compromised. The vital signs are as follows: blood pressure, 180/100 mm Hg; heart rate, 59/min; respiratory rate, 12/min; temperature 37.0℃ (98.6℉); and SaO2, 96% on room air. The examination revealed bruising in the right frontotemporal region. The pupils are round, equal, and show a poor response to light. The neurologic examination shows hyperreflexia and decreased power in the left upper and lower limbs. There is questionable nuchal rigidity, but no Kernig and Brudzinski signs. The CT scan is shown in the image. Which of the following options is recommended for this patient?
A mass casualty incident occurs with 25 casualties arriving simultaneously at a community hospital emergency department. The trauma team has limited resources with 2 operating rooms available and 4 surgeons present. Among the arriving patients: Patient A has traumatic amputation of forearm with tourniquet in place and stable vitals; Patient B has flail chest, respiratory distress, and unstable vitals; Patient C is in cardiac arrest with penetrating chest wound; Patient D has a femur fracture with stable vitals; Patient E has GCS 4 with bilateral blown pupils. Evaluate the triage priority according to ATLS mass casualty protocols.
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app