
Perioperative respiratory management — MCQs

A 21-year-old man undergoes orthopedic surgery for a leg fracture that he has sustained in a motorbike accident. After induction of anesthesia with desflurane, the patient's respiratory minute ventilation decreases notably. Which of the following additional effects is most likely to occur in response to this drug?
A 56-year-old previously healthy woman with no other past medical history is post-operative day one from an open reduction and internal fixation of a fractured right radius and ulna after a motor vehicle accident. What is one of the primary ways of preventing postoperative pneumonia in this patient?
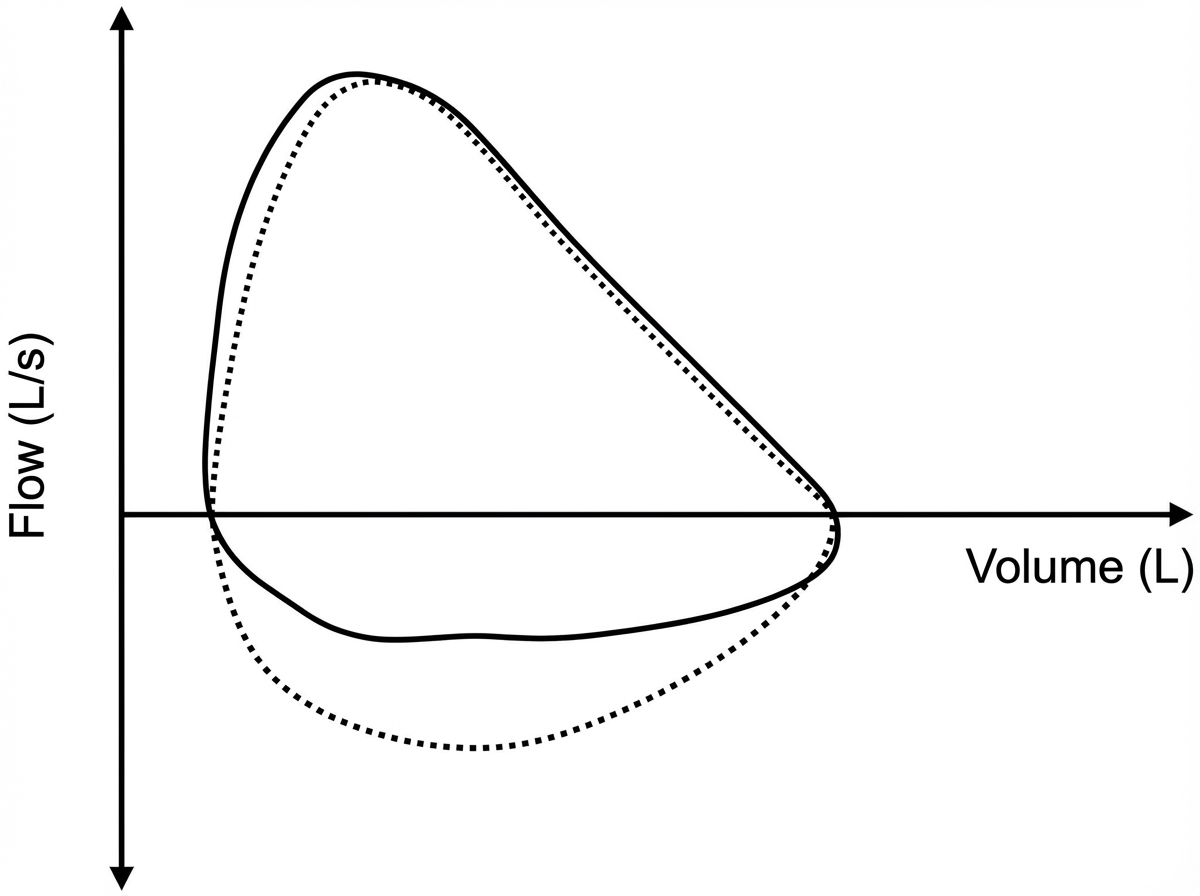
Five minutes after arriving in the postoperative care unit following total knee replacement under general anesthesia, a 55-year-old woman is acutely short of breath. The procedure was uncomplicated. Postoperatively, prophylactic treatment with cefazolin was begun and the patient received morphine and ketorolac for pain management. She has generalized anxiety disorder. Her only other medication is escitalopram. She has smoked one pack of cigarettes daily for 25 years. Her temperature is 37°C (98.6°F), pulse is 108/min, respirations are 26/min, and blood pressure is 95/52 mm Hg. A flow-volume loop obtained via pulmonary function testing is shown. Which of the following is the most likely underlying cause of this patient's symptoms?
A 57-year-old man presents to the clinic for a chronic cough over the past 4 months. The patient reports a productive yellow/green cough that is worse at night. He denies any significant precipitating event prior to his symptoms. He denies fever, chest pain, palpitations, weight changes, or abdominal pain, but endorses some difficulty breathing that waxes and wanes. He denies alcohol usage but endorses a 35 pack-year smoking history. A physical examination demonstrates mild wheezes, bibasilar crackles, and mild clubbing of his fingertips. A pulmonary function test is subsequently ordered, and partial results are shown below: Tidal volume: 500 mL Residual volume: 1700 mL Expiratory reserve volume: 1500 mL Inspiratory reserve volume: 3000 mL What is the functional residual capacity of this patient?
A 23-year-old man is admitted to the intensive care unit with acute respiratory distress syndrome (ARDS) due to influenza A. He has no history of serious illness and does not smoke. An x-ray of the chest shows diffuse bilateral infiltrates. Two weeks later, his symptoms have improved. Pulmonary examination on discharge shows inspiratory crackles at both lung bases. This patient is most likely to develop which of the following long-term complications?
A 63-year-old man undergoes workup for nocturnal dyspnea and what he describes as a "choking" sensation while sleeping. He also endorses fatigue and dyspnea on exertion. Physical exam reveals a normal S1, loud P2, and a neck circumference of 17 inches (43 cm) (normal < 14 inches (< 35 cm)). His temperature is 98.8°F (37°C), blood pressure is 128/82 mmHg, pulse is 86/min, and respirations are 19/min. He undergoes spirometry, which is unrevealing, and polysomnography, which shows 16 hypopneic and apneic events per hour. Mean pulmonary arterial pressure is 30 mmHg. Which of the following complications is this patient most at risk for?
A 34-year-old man comes to the physician for a follow-up examination. He has a 3-month history of a nonproductive cough. He has been treated with diphenhydramine since his last visit 2 weeks ago, but his symptoms have persisted. He does not smoke. He drinks 3 beers on the weekends. He is 177 cm (5 ft 10 in) tall and weighs 100 kg (220.46 lbs); BMI is 35.1 kg/m2. His temperature is 37.1°C (98.8°F), pulse is 78/min, respirations are 14/min, and blood pressure is 130/80 mm Hg. Pulse oximetry on room air shows an oxygen saturation of 97%. Physical examination and an x-ray of the chest show no abnormalities. Which of the following is the most appropriate next step in management?
A 63-year-old man presents to the clinic complaining of burning bilateral leg pain which has been increasing gradually over the past several months. It worsens when he walks but improves with rest. His past medical and surgical history are significant for hypertension, hyperlipidemia, diabetes, and a 40-pack-year smoking history. His temperature is 99.0°F (37.2°C), blood pressure is 167/108 mm Hg, pulse is 88/min, respirations are 13/min, and oxygen saturation is 95% on room air. Physical exam of the lower extremities reveals palpable but weak posterior tibial and dorsalis pedis pulses bilaterally. Which of the following is the best initial treatment for this patient's symptoms?
An obese 52-year-old man is brought to the emergency department because of increasing shortness of breath for the past 8 hours. Two months ago, he noticed a mass on the right side of his neck and was diagnosed with laryngeal cancer. He has smoked two packs of cigarettes daily for 27 years. He drinks two pints of rum daily. He appears ill. He is oriented to person, place, and time. His temperature is 37°C (98.6°F), pulse is 111/min, respirations are 34/min, and blood pressure is 140/90 mm Hg. Pulse oximetry on room air shows an oxygen saturation of 89%. Examination shows a 9-cm, tender, firm subglottic mass on the right side of the neck. Cervical lymphadenopathy is present. His breathing is labored and he has audible inspiratory stridor but is able to answer questions. The lungs are clear to auscultation. Arterial blood gas analysis on room air shows: pH 7.36 PCO2 45 mm Hg PO2 74 mm Hg HCO3- 25 mEq/L He has no advanced directive. Which of the following is the most appropriate next step in management?
A 47-year-old man is brought to the emergency room by his wife. She states that they were having dinner at a restaurant when the patient suddenly became out of breath. His past medical history is irrelevant but has a 20-year pack smoking history. On evaluation, the patient is alert and verbally responsive but in moderate respiratory distress. His temperature is 37°C (98.6°F), blood pressure is 85/56 mm Hg, pulse is 102/min, and respirations are 20/min. His oxygen saturation is 88% on 2L nasal cannula. An oropharyngeal examination is unremarkable. The trachea is deviated to the left. Cardiopulmonary examination reveals decreased breath sounds on the right lower lung field with nondistended neck veins. Which of the following is the next best step in the management of this patient?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app