
Small bowel obstruction — MCQs

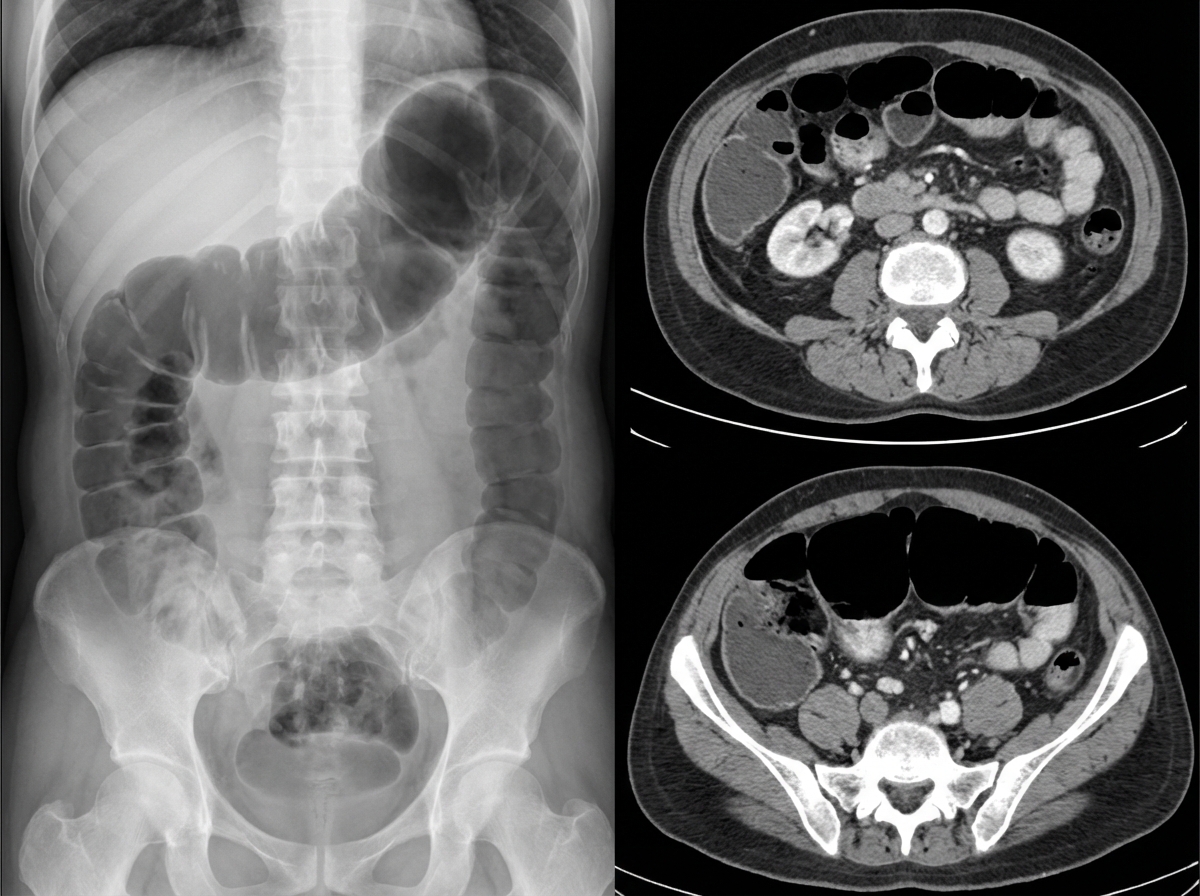
A 69-year-old male presents to the Emergency Department with bilious vomiting that started within the past 24 hours. His medical history is significant for hypertension, hyperlipidemia, and a myocardial infarction six months ago. His past surgical history is significant for a laparotomy 20 years ago for a perforated diverticulum. Most recently he had some dental work done and has been on narcotic pain medicine for the past week. He reports constipation and obstipation. He is afebrile with a blood pressure of 146/92 mm Hg and a heart rate of 116/min. His abdominal exam reveals multiple well-healed scars with distension but no tenderness. An abdominal/pelvic CT scan reveals dilated small bowel with a transition point to normal caliber bowel distally. When did the cause of his pathology commence?
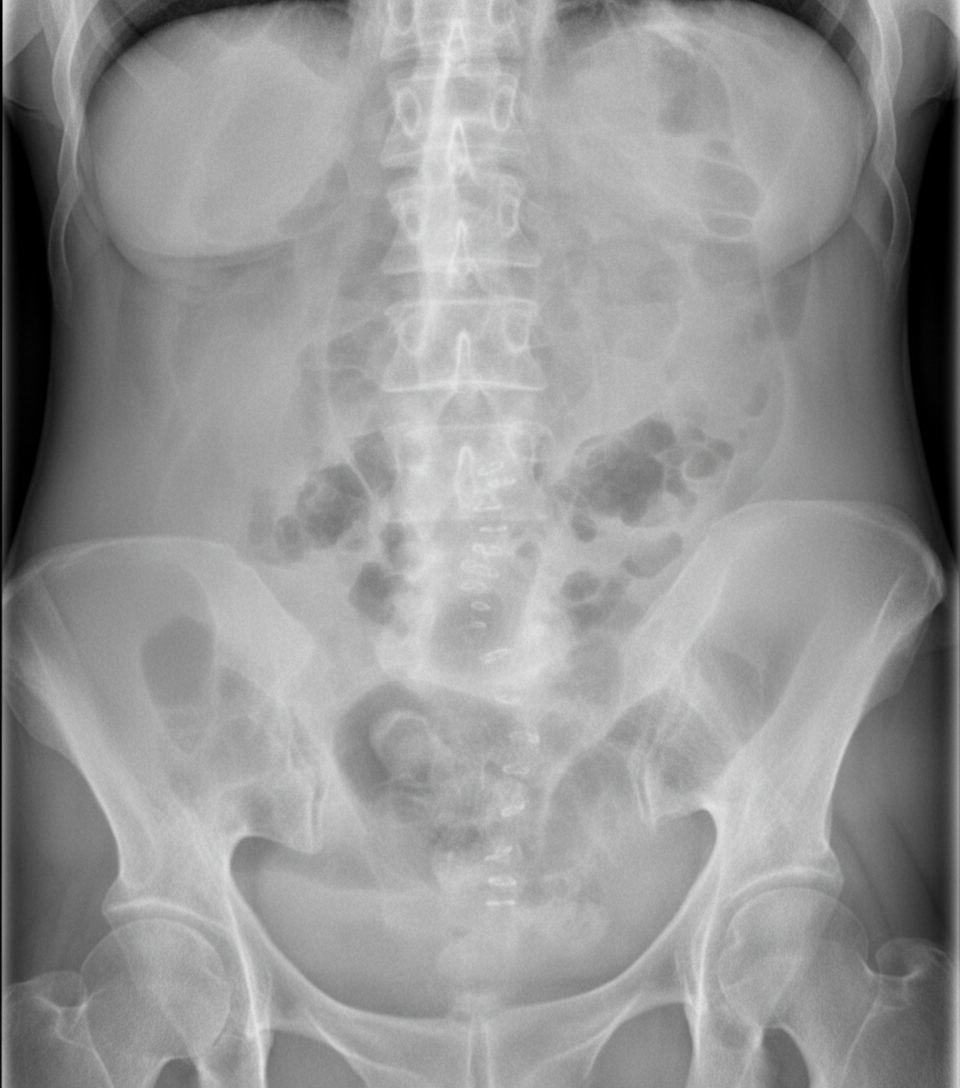
A 76-year-old female is brought to the emergency department after being found unresponsive in her room at her nursing facility. Past medical history is significant for Alzheimer's disease, hypertension, and diabetes. Surgical history is notable for an open cholecystectomy at age 38 and multiple cesarean sections. On arrival, she is non-responsive but breathing by herself, and her vital signs are T 102.9 F, HR 123 bpm, BP 95/64, RR 26/min, and SaO2 97% on 6L nasal cannula. On physical exam the patient has marked abdominal distension and is tympanic to percussion. Laboratory studies are notable for a lactic acidosis. An upright abdominal radiograph and CT abdomen/pelvis with contrast are shown in Figures A and B respectively. She is started on IV fluids and a nasogastric tube is placed to suction which returns green bilious fluid. Repeat vitals 1 hour later are T 101F, HR 140 bpm, BP 75/44, RR 30/min, and SaO2 is 100% on the ventilator after she is intubated for airway concerns. What is the next best step in management?
A 68-year-old woman is brought to the emergency department with intense abdominal pain for the past 2 hours. She has had 1 episode of bloody diarrhea recently. She has an 18-year history of diabetes mellitus. She was diagnosed with hypertension and ischemic heart disease 6 years ago. She is fully alert and oriented. Her temperature is 37.5°C (99.5°F), blood pressure is 145/90 mm Hg, pulse is 78/min, and respirations are 14/min. Abdominal examination shows mild generalized abdominal tenderness without guarding or rebound tenderness. An abdominal plain X-ray shows no abnormalities. Abdominal CT reveals colonic wall thickening and pericolonic fat stranding in the splenic curvature. Bowel rest, intravenous hydration, and IV antibiotics are initiated. Which of the following is the most important diagnostic evaluation at this time?
A 54-year-old man comes to the physician because of diarrhea that has become progressively worse over the past 4 months. He currently has 4–6 episodes of foul-smelling stools per day. Over the past 3 months, he has had fatigue and a 5-kg (11-lb) weight loss. He returned from Bangladesh 6 months ago after a year-long business assignment. He has osteoarthritis and hypertension. Current medications include amlodipine and naproxen. He appears pale and malnourished. His temperature is 37.3°C (99.1°F), pulse is 76/min, and blood pressure is 140/86 mm Hg. Examination shows pale conjunctivae and dry mucous membranes. Angular stomatitis and glossitis are present. The abdomen is distended but soft and nontender. Rectal examination shows no abnormalities. Laboratory studies show: Hemoglobin 8.9 g/dL Leukocyte count 4100/mm3 Platelet count 160,000/mm3 Mean corpuscular volume 110 μm3 Serum Na+ 133 mEq/L Cl- 98 mEq/l K+ 3.3 mEq/L Creatinine 1.1 mg/dL IgA 250 mg/dL Anti-tissue transglutaminase, IgA negative Stool culture and studies for ova and parasites are negative. Test of the stool for occult blood is negative. Fecal fat content is 22 g/day (N < 7). Fecal lactoferrin is negative and elastase is within normal limits. Which of the following is the most appropriate next step in diagnosis?
A 75-year-old man is brought to the emergency department after 2 days of severe diffuse abdominal pain, nausea, vomiting, and lack of bowel movements, which has led him to stop eating. He has a history of type-2 diabetes mellitus, hypertension, and chronic obstructive pulmonary disease. Upon admission, his vital signs are within normal limits and physical examination shows diffuse abdominal tenderness, distention, lack of bowel sounds, and an empty rectal ampulla. After initial fluid therapy and correction of moderate hypokalemia, the patient's condition shows mild improvement. His abdominal plain film is taken and shown. Which of the following is the most appropriate concomitant approach?
A 55-year-old woman comes to the emergency department because of a 24-hour history of severe lower abdominal pain. She has had two episodes of nonbloody vomiting today and has been unable to keep down food or fluids. She has not had a bowel movement since the day before. She has hypertension, hyperlipidemia, and osteoarthritis. She had a cholecystectomy 5 years ago. She has smoked one pack of cigarettes daily for the last 20 years. Current medications include chlorthalidone, atorvastatin, and naproxen. Her temperature is 38.8°C (101.8°F), pulse is 102/min, respirations are 20/min, and blood pressure is 118/78 mm Hg. She is 1.68 m (5 ft 6 in) tall and weighs 94.3 kg (207.9 lbs); BMI is 33.4 kg/m2. Abdominal examination shows a soft abdomen with hypoactive bowel sounds. There is moderate left lower quadrant tenderness. A tender mass is palpable on digital rectal examination. There is no guarding or rebound tenderness. Laboratory studies show: Leukocyte count 17,000/mm3 Hemoglobin 13.3 g/dl Hematocrit 40% Platelet count 188,000/mm3 Serum Na+ 138 mEq/L K+ 4.1 mEq/L Cl- 101 mEq/L HCO3- 22 mEq/L Urea Nitrogen 18.1 mg/dl Creatinine 1.1 mg/dl Which of the following is most appropriate to confirm the diagnosis?
A 55-year-old man presents to the emergency department with nausea and vomiting. The patient states that he has felt nauseous for the past week and began vomiting last night. He thought his symptoms would resolve but decided to come in when his symptoms worsened. He feels that his symptoms are exacerbated with large fatty meals and when he drinks alcohol. His wife recently returned from a cruise with symptoms of vomiting and diarrhea. The patient has a past medical history of poorly managed diabetes, constipation, anxiety, dyslipidemia, and hypertension. His temperature is 99.5°F (37.5°C), blood pressure is 197/128 mmHg, pulse is 100/min, respirations are 17/min, and oxygen saturation is 95% on room air. Physical exam reveals a systolic murmur heard loudest along the left upper sternal border. Abdominal exam reveals an obese, tympanitic and distended abdomen with a 3 cm scar in the right lower quadrant. Vascular exam reveals weak pulses in the lower extremities. Which of the following is the most likely diagnosis?
A 73-year-old man presents to the emergency department complaining of abdominal pain with nausea and vomiting, stating that he “can’t keep anything down”. He states that the pain has been gradually getting worse over the past 2 months, saying that, at first, it was present only an hour after he ate but now is constant. He also says that he has been constipated for the last 2 weeks, which has also been getting progressively worse. His last bowel movement was 4 days ago which was normal. He states that he cannot pass flatus. The patient’s past medical history is significant for hypertension and an episode of pneumonia last year. The patient is afebrile and his pulse is 105/min. On physical examination, the patient is uncomfortable. His lungs are clear to auscultation bilaterally. His abdomen is visibly distended and diffusely tender with tympany on percussion. A contrast CT scan of the abdomen shows dilated loops of small bowel with collapsed large bowel. Which of the following is the most likely cause of this patient’s condition?
A 32-year-old man comes to the emergency department because of recurrent episodes of vomiting for 1 day. He has had over 15 episodes of bilious vomiting. During this period he has had cramping abdominal pain but has not had a bowel movement or passed flatus. He does not have fever or diarrhea. He was diagnosed with Crohn disease at the age of 28 years which has been well controlled with oral mesalamine. He underwent a partial small bowel resection for midgut volvulus at birth. His other medications include vitamin B12, folic acid, loperamide, ferrous sulfate, and vitamin D3. He appears uncomfortable and his lips are parched. His temperature is 37.1°C (99.3°F), pulse is 103/min, and blood pressure is 104/70 mm Hg. The abdomen is distended, tympanitic, and tender to palpation over the periumbilical area and the right lower quadrant. Rectal examination is unremarkable. A CT scan of the abdomen shows multiple dilated loops of small bowel with a transition zone in the mid to distal ileum. After 24 hours of conservative management with IV fluid resuscitation, nasogastric bowel decompression, promethazine, and analgesia, his condition does not improve and a laparotomy is scheduled. During the laparotomy, two discrete strictures are noted in the mid-ileum, around 20 cm apart. Which of the following is the most appropriate next step in management?
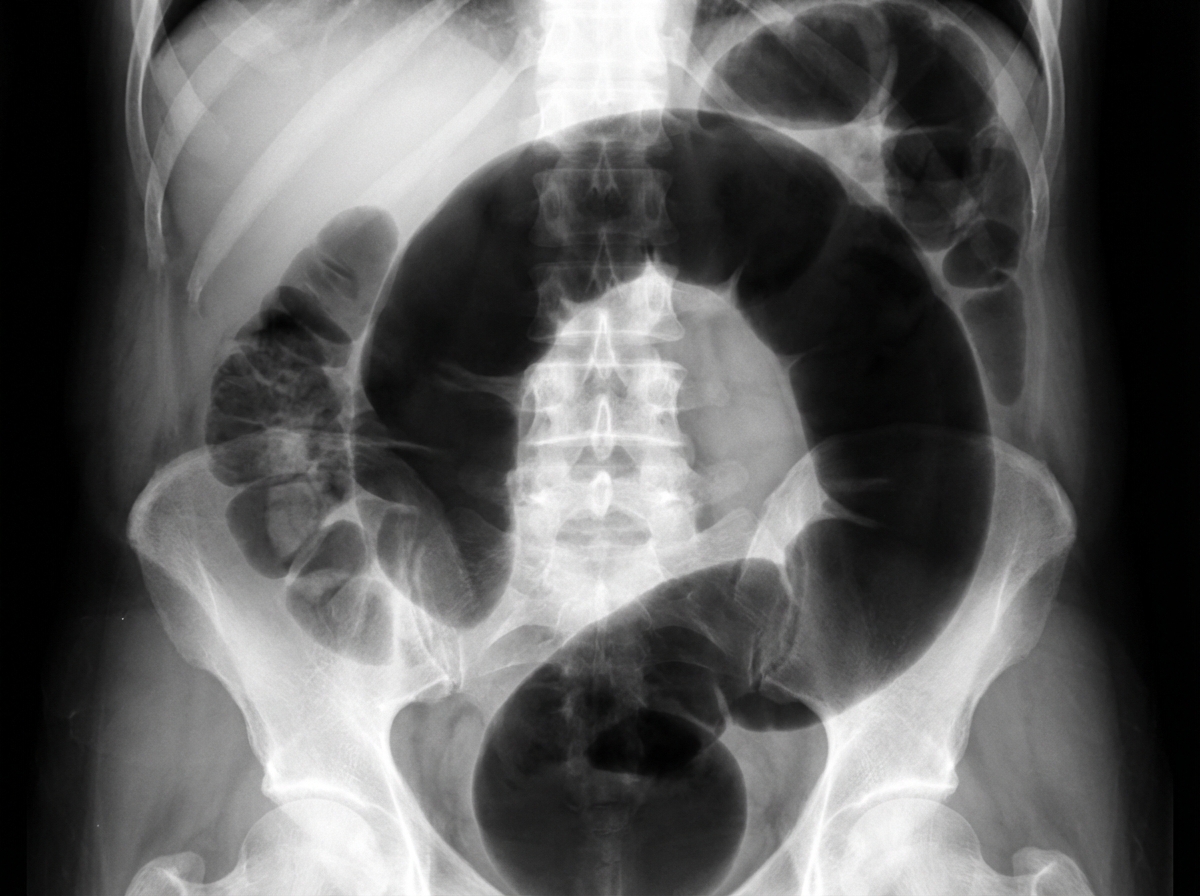
An institutionalized 65-year-old man is brought to the emergency department because of abdominal pain and distension for 12 hours. The pain was acute in onset and is a cramping-type pain associated with nausea, vomiting, and constipation. He has a history of chronic constipation and has used laxatives for years. There is no history of inflammatory bowel disease in his family. He has not been hospitalized recently. There is no recent history of weight loss or change in bowel habits. On physical examination, the patient appears ill. The abdomen is distended with tenderness mainly in the left lower quadrant and is tympanic on percussion. The blood pressure is 110/79 mm Hg, heart rate is 100/min, the respiratory rate is 20/min, and the temperature is 37.2°C (99.0°F). The CBC shows an elevated white blood cell count. The plain abdominal X-ray is shown in the accompanying image. What is the most likely cause of his condition?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app