
Abdominal emergencies — MCQs

On this page
A 57-year-old man presents to the office with complaints of perianal pain during defecation and perineal heaviness for 1 month. He also complains of discharge around his anus, and bright red bleeding during defecation. The patient provides a history of having a sexual relationship with other men without using any methods of protection. The physical examination demonstrates edematous verrucous anal folds that are of hard consistency and painful to the touch. A proctosigmoidoscopy reveals an anal canal ulcer with well defined, indurated borders on a white background. A biopsy is taken and the results are pending. What is the most likely diagnosis?
An 18-year-old woman presents to the emergency department with severe right lower quadrant discomfort and stomach pain for the past day. She has no significant past medical history. She states that she is sexually active and uses oral contraceptive pills for birth control. Her vital signs include: blood pressure 127/81 mm Hg, pulse 101/min, respiratory rate 19/min, and temperature 39.0°C (102.2°F). Abdominal examination is significant for focal tenderness and guarding in the right lower quadrant. Blood is drawn for lab tests which reveal the following: Hb% 13 gm/dL Total count (WBC) 15,400 /mm3 Differential count Neutrophils: Segmented 70% Band Form 5% Lymphocytes 20% Monocytes 5% What is the next best step in the management of this patient?
A 50-year-old male presents to the emergency with abdominal pain. He reports he has had abdominal pain associated with meals for several months and has been taking over the counter antacids as needed, but experienced significant worsening pain one hour ago in the epigastric region. The patient reports the pain radiating to his shoulders. Vital signs are T 38, HR 120, BP 100/60, RR 18, SpO2 98%. Physical exam reveals diffuse abdominal rigidity with rebound tenderness. Auscultation reveals hypoactive bowel sounds. Which of the following is the next best step in management?
A 71-year-old man with hypertension is taken to the emergency department after the sudden onset of stabbing abdominal pain that radiates to the back. He has smoked 1 pack of cigarettes daily for 20 years. His pulse is 120/min and thready, respirations are 18/min, and blood pressure is 82/54 mm Hg. Physical examination shows a periumbilical, pulsatile mass and abdominal bruit. There is epigastric tenderness. Which of the following is the most likely underlying mechanism of this patient's current condition?
A 42-year-old woman presents to the emergency department with abdominal pain. Her pain started last night during dinner and has persisted. This morning, the patient felt very ill and her husband called emergency medical services. The patient has a past medical history of obesity, diabetes, and depression. Her temperature is 104°F (40°C), blood pressure is 90/65 mmHg, pulse is 160/min, respirations are 14/min, and oxygen saturation is 98% on room air. Physical exam is notable for a very ill appearing woman. Her skin is mildly yellow, and she is in an antalgic position on the stretcher. Laboratory values are ordered as seen below. Hemoglobin: 13 g/dL Hematocrit: 38% Leukocyte count: 14,500 cells/mm^3 with normal differential Platelet count: 257,000/mm^3 Alkaline phosphatase: 227 U/L Bilirubin, total: 11.3 mg/dL Bilirubin, direct: 9.8 mg/dL AST: 42 U/L ALT: 31 U/L The patient is started on antibiotics and IV fluids. Which of the following is the best next step in management?
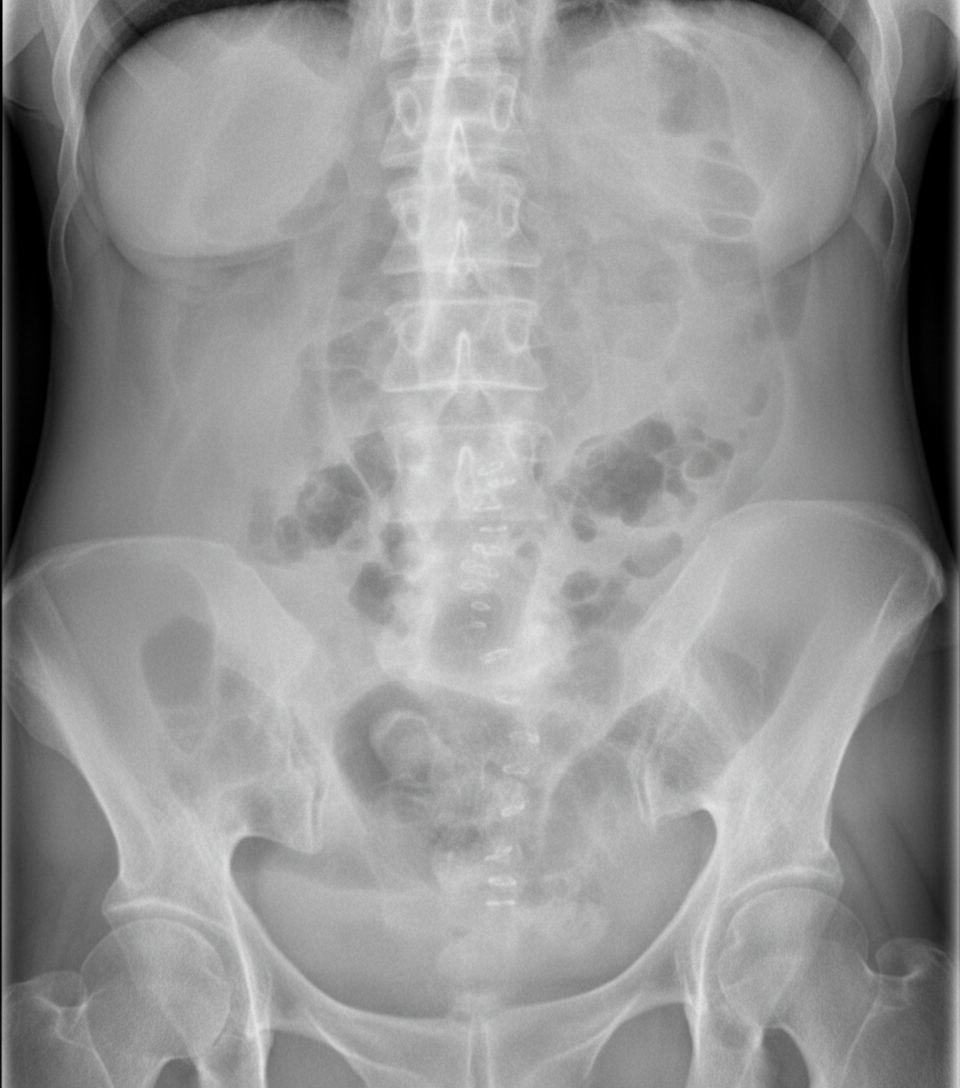
A 68-year-old man is brought to the emergency department for increasing colicky lower abdominal pain and distention for 4 days. He has nausea. He has not passed flatus for the past 2 days. His last bowel movement was 4 days ago. He has hypertension, type 2 diabetes mellitus, and left hemiplegia due to a cerebral infarction that occurred 2 years ago. His current medications include aspirin, atorvastatin, hydrochlorothiazide, enalapril, and insulin. His temperature is 37.3°C (99.1°F), pulse is 90/min, and blood pressure is 126/84 mm Hg. Examination shows a distended and tympanitic abdomen. There is mild tenderness to palpation over the lower abdomen. Bowel sounds are decreased. Digital rectal examination shows an empty rectum. Muscle strength is decreased in the left upper and lower extremities. Deep tendon reflexes are 3+ on the left and 2+ on the right. The remainder of the examination shows no abnormalities. Laboratory studies are within normal limits. A frontal x-ray of the abdomen is shown. The patient is kept nil per os and a nasogastric tube is inserted. Intravenous fluids are administered. Which of the following is the most appropriate next step in the management of this patient?

A 37-year-old woman comes to the physician because of right-sided inguinal pain for the past 8 weeks. During this period, the patient has had increased pain during activities such as walking and standing. She has no nausea, vomiting, or fever. Her temperature is 36.8°C (98.2°F), pulse is 73/min, and blood pressure is 132/80 mm Hg. The abdomen is soft and nontender. There is a visible and palpable groin protrusion above the inguinal ligament on the right side. Bulging is felt during Valsalva maneuver. Which of the following is the most likely diagnosis?
A 30-year-old woman, gravida 1, para 0, at 30 weeks' gestation is brought to the emergency department because of progressive upper abdominal pain for the past hour. The patient vomited once on her way to the hospital. She said she initially had dull, generalized stomach pain about 6 hours prior, but now the pain is located in the upper abdomen and is more severe. There is no personal or family history of any serious illnesses. She is sexually active with her husband. She does not smoke or drink alcohol. Medications include folic acid and a multivitamin. Her temperature is 38.5°C (101.3°F), pulse is 100/min, and blood pressure is 130/80 mm Hg. Physical examination shows right upper quadrant tenderness. The remainder of the examination shows no abnormalities. Laboratory studies show a leukocyte count of 12,000/mm3. Urinalysis shows mild pyuria. Which of the following is the most appropriate definitive treatment in the management of this patient?
A 75-year-old man is brought to the emergency department after 2 days of severe diffuse abdominal pain, nausea, vomiting, and lack of bowel movements, which has led him to stop eating. He has a history of type-2 diabetes mellitus, hypertension, chronic obstructive pulmonary disease, and an open cholecystectomy performed 5 days ago. Upon admission, his vital signs are within normal limits and physical examination shows diffuse abdominal tenderness, distention, lack of bowel sounds, and an empty rectal ampulla. After initial fluid therapy and correction of moderate hypokalemia, the patient's condition shows mild improvement. His abdominal plain film is taken and shown. Which of the following is the most appropriate concomitant approach?
A 33-year-old woman comes to the emergency department because of severe right flank pain for 2 hours. The pain is colicky in nature and she describes it as 9 out of 10 in intensity. She has had 2 episodes of vomiting. She has no history of similar episodes in the past. She is 160 cm (5 ft 3 in) tall and weighs 104 kg (229 lb); BMI is 41 kg/m2. Her temperature is 37.3°C (99.1°F), pulse is 96/min, respirations are 16/min and blood pressure is 116/76 mm Hg. The abdomen is soft and there is mild tenderness to palpation in the right lower quadrant. Bowel sounds are reduced. The remainder of the examination shows no abnormalities. Her leukocyte count is 7,400/mm3. A low-dose CT scan of the abdomen and pelvis shows a round 12-mm stone in the distal right ureter. Urine dipstick is mildly positive for blood. Microscopic examination of the urine shows RBCs and no WBCs. 0.9% saline infusion is begun and intravenous ketorolac is administered. Which of the following is the most appropriate next step in management?
Practice by Chapter
Acute appendicitis
Practice Questions
Acute cholecystitis
Practice Questions
Small bowel obstruction
Practice Questions
Large bowel obstruction
Practice Questions
Mesenteric ischemia
Practice Questions
Gastrointestinal perforation
Practice Questions
Abdominal compartment syndrome
Practice Questions
Acute pancreatitis management
Practice Questions
Diverticulitis
Practice Questions
Incarcerated/strangulated hernias
Practice Questions
Non-operative management principles
Practice Questions
Diagnostic approach to acute abdomen
Practice Questions
Damage control surgery
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app