
Abdominal emergencies — MCQs

On this page
A 38-year-old man arrives at the emergency department with severe periumbilical, colicky pain and abdominal distention for the past 2 days. He is nauseated and reports vomiting light-green emesis 8 times since yesterday morning. He has not had a bowel movement or passed any gas for the past 3 days. He has a past medical history of ventral hernia repair 5 years ago. His heart rate is 110/min, respiratory rate is 24/min, temperature is 38.0°C (100.4°F), and blood pressure is 120/90 mm Hg. The abdomen is distended and mildly tender to deep palpation. Bowel sounds are high-pitched and tinkling. Which of the following is the most likely cause?
A 48-year-old woman with a history of obesity presents with acute onset of diffuse epigastric pain that began a few hours ago and then localized to the right upper quadrant. Further questioning reveals that the pain has been exacerbated by eating but has otherwise been unchanged in nature. Physical exam reveals severe right upper quadrant pain that is accompanied by arrest of respiration with deep palpation of the right upper quadrant. Which of the following symptoms is associated with the most likely etiology of this patient's presentation?
A 28-year-old woman presents for her annual physical examination. She describes a painless lump in her left breast detected during breast self-examination two weeks ago. She has no previous history of breast lumps and considers herself to be generally healthy. She takes no medication and does not smoke tobacco or drink alcohol. The patient has no personal or family history of breast cancer. Her vitals are normal. Physical examination reveals a firm, 1 to 2 cm mass in the lateral aspect of her left breast. However, no associated skin changes, nipple discharge, or retraction are found. No axillary adenopathy is present. What is the most appropriate next step in the workup of this patient?
A 27-year-old-man is brought to the emergency department 30 minutes after being involved in a motorcycle accident. He lost control at high speed and was thrown forward onto the handlebars. On arrival, he is alert and responsive. He has abdominal pain and superficial lacerations on his left arm. Vital signs are within normal limits. Examination shows a tender, erythematous area over his epigastrium. The abdomen is soft and non-distended. A CT scan of the abdomen shows no abnormalities. Treatment with analgesics is begun, the lacerations are cleaned and dressed, and the patient is discharged home after 2 hours of observation. Four days later, the patient returns to the emergency department with gradually worsening upper abdominal pain, fever, poor appetite, and vomiting. His pulse is 91/min and blood pressure is 135/82 mm Hg. Which of the following is the most likely diagnosis?
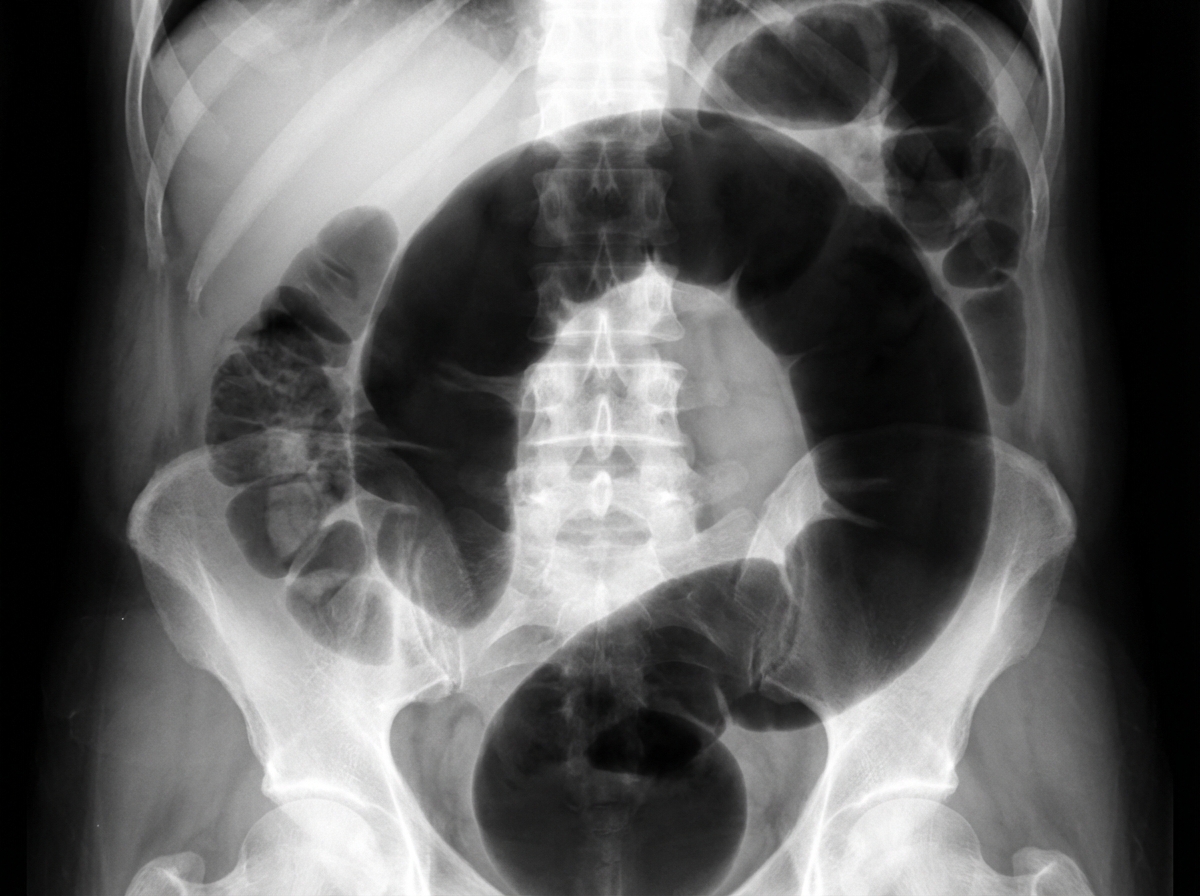
An institutionalized 65-year-old man is brought to the emergency department because of abdominal pain and distension for 12 hours. The pain was acute in onset and is a cramping-type pain associated with nausea, vomiting, and constipation. He has a history of chronic constipation and has used laxatives for years. There is no history of inflammatory bowel disease in his family. He has not been hospitalized recently. There is no recent history of weight loss or change in bowel habits. On physical examination, the patient appears ill. The abdomen is distended with tenderness mainly in the left lower quadrant and is tympanic on percussion. The blood pressure is 110/79 mm Hg, heart rate is 100/min, the respiratory rate is 20/min, and the temperature is 37.2°C (99.0°F). The CBC shows an elevated white blood cell count. The plain abdominal X-ray is shown in the accompanying image. What is the most likely cause of his condition?
During the course of investigation of a suspected abdominal aortic aneurysm in a 57-year-old woman, a solid 6 × 5 cm mass is detected in the right kidney. The abdominal aorta reveals no abnormalities. The patient is feeling well and has no history of any serious illness or medication usage. She is a 25-pack-year smoker. Her vital signs are within normal limits. Physical examination reveals no abnormalities. Biopsy of the mass shows renal cell carcinoma. Contrast-enhanced CT scan indicates no abnormalities involving contralateral kidney, lymph nodes, lungs, liver, bone, or brain. Which of the following treatment options is the most appropriate next step in the management of this patient?
A 72-year-old female presents to the emergency department complaining of severe abdominal pain and several days of bloody diarrhea. Her symptoms began with intermittent bloody diarrhea five days ago and have worsened steadily. For the last 24 hours, she has complained of fevers, chills, and abdominal pain. She has a history of ulcerative colitis, idiopathic hypertension, and hypothyroidism. Her medications include hydrochlorothiazide, levothyroxine, and sulfasalazine. In the ED, her temperature is 39.1°C (102.4°F), pulse is 120/min, blood pressure is 90/60 mmHg, and respirations are 20/min. On exam, the patient is alert and oriented to person and place, but does not know the day. Her mucus membranes are dry. Heart and lung exam are not revealing. Her abdomen is distended with marked rebound tenderness. Bowel sounds are hyperactive. Serum: Na+: 142 mEq/L Cl-: 107 mEq/L K+: 3.3 mEq/L HCO3-: 20 mEq/L BUN: 15 mg/dL Glucose: 92 mg/dL Creatinine: 1.2 mg/dL Calcium: 10.1 mg/dL Hemoglobin: 11.2 g/dL Hematocrit: 30% Leukocyte count: 14,600/mm^3 with normal differential Platelet count: 405,000/mm^3 What is the next best step in management?
A 55-year-old man presents to the emergency department with nausea and vomiting. The patient states that he has felt nauseous for the past week and began vomiting last night. He thought his symptoms would resolve but decided to come in when his symptoms worsened. He feels that his symptoms are exacerbated with large fatty meals and when he drinks alcohol. His wife recently returned from a cruise with symptoms of vomiting and diarrhea. The patient has a past medical history of poorly managed diabetes, constipation, anxiety, dyslipidemia, and hypertension. His temperature is 99.5°F (37.5°C), blood pressure is 197/128 mmHg, pulse is 100/min, respirations are 17/min, and oxygen saturation is 95% on room air. Physical exam reveals a systolic murmur heard loudest along the left upper sternal border. Abdominal exam reveals an obese, tympanitic and distended abdomen with a 3 cm scar in the right lower quadrant. Vascular exam reveals weak pulses in the lower extremities. Which of the following is the most likely diagnosis?
A 38-year-old man comes to the physician because of a 2-week history of severe pain while passing stools. The stools are covered with bright red blood. He has been avoiding defecation because of the pain. Last year, he was hospitalized for pilonidal sinus surgery. He has had chronic lower back pain ever since he had an accident at his workplace 10 years ago. The patient's father was diagnosed with colon cancer at the age of 62. Current medications include oxycodone and gabapentin. He is 163 cm (5 ft 4 in) tall and weighs 100 kg (220 lb); BMI is 37.6 kg/m2. Vital signs are within normal limits. The abdomen is soft and nontender. Digital rectal examination was not performed because of severe pain. His hemoglobin is 16.3 mg/dL and his leukocyte count is 8300/mm3. Which of the following is the most appropriate next step in management?
A 26-year-old woman presents to her primary care physician for 5 days of increasing pelvic pain. She says that the pain has been present for the last 2 months; however, it has become increasingly severe recently. She also says that the pain has been accompanied by unusually heavy menstrual periods in the last few months. Physical exam reveals a mass in the right adnexa, and ultrasonography reveals a 9 cm right ovarian mass. If this mass is surgically removed, which of the following structures must be diligently protected?
Practice by Chapter
Acute appendicitis
Practice Questions
Acute cholecystitis
Practice Questions
Small bowel obstruction
Practice Questions
Large bowel obstruction
Practice Questions
Mesenteric ischemia
Practice Questions
Gastrointestinal perforation
Practice Questions
Abdominal compartment syndrome
Practice Questions
Acute pancreatitis management
Practice Questions
Diverticulitis
Practice Questions
Incarcerated/strangulated hernias
Practice Questions
Non-operative management principles
Practice Questions
Diagnostic approach to acute abdomen
Practice Questions
Damage control surgery
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app