
Abdominal emergencies — MCQs

On this page
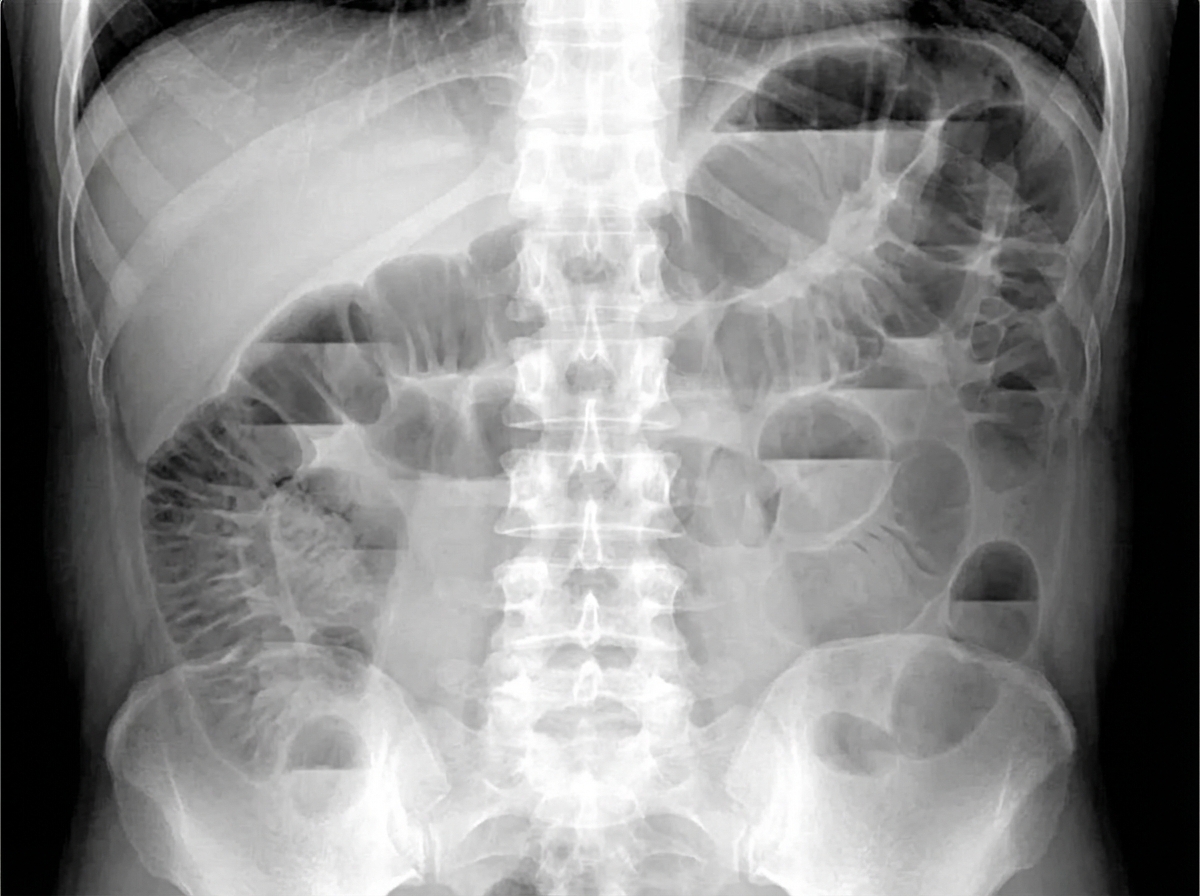
A 42-year-old man on postoperative day 2 after an uncomplicated abdominal operation has persistent nausea, bilious vomiting, and diffuse abdominal distension. His temperature is 37.0°C (98.6°F), blood pressure is 122/74 mm Hg, and pulse is 86/min. The abdomen is distended with hypoactive bowel sounds and mild diffuse tenderness but no guarding or rebound. Laboratory studies show no leukocytosis or metabolic acidosis. The upright abdominal radiograph shown demonstrates diffuse gaseous dilation of both small and large bowel, with residual enteric contrast and gas extending throughout the colon and no free intraperitoneal air. Which of the following is the most appropriate initial management?
A 24-year-old woman with a past medical history significant only for endometriosis presents to the outpatient clinic with a 2-cm left breast mass that she first identified 6 months earlier. On review of systems, the patient states that the mass is not painful and, by her estimation, has not significantly increased in size since she first noticed it. On physical examination, there is a palpable, round, rubbery, mobile mass approximately 2 cm in diameter. Given the lesion’s characteristics and the patient’s demographics, what is the most likely diagnosis?
A 40-year-old female visits the emergency department with right upper quadrant pain and fever of 2-hours duration. She denies alcohol, cigarette, and drug use and reports no other medical problems. Body mass index is 30 kg/m^2. Her temperature is 38.5 degrees Celsius (101.3 degrees Fahrenheit), blood pressure is 130/80 mm Hg, pulse is 90/min, and respirations are 18/min. Jaundice is present in the sclera and at the base of the tongue. The abdomen is tender in the right upper quadrant. Liver function test (LFTs) reveal elevated direct and total bilirubin and alkaline phosphatase of 500 U/L. IV Ampicillin-gentamicin is administered, fluid resuscitation is initiated, and over 24 hours the patient’s fever improves. Which of the following is the next step in the management of this patient:
A 49-year-old man comes to the emergency department because of recurrent abdominal pain for 1 week. The pain is worse after eating and he has vomited twice during this period. He was hospitalized twice for acute pancreatitis during the past year; the latest being 2 months ago. There is no family history of serious illness. His only medication is a vitamin supplement. He has a history of drinking five beers a day for several years but quit 1 month ago. His temperature is 37.1°C (98.8°F), pulse is 98/min and blood pressure 110/70 mm Hg. He appears uncomfortable. Examination shows epigastric tenderness to palpation; there is no guarding or rebound. A CT scan of the abdomen shows a 6-cm low attenuation oval collection with a well-defined wall contiguous with the body of the pancreas. Which of the following is the most appropriate next step in management?
A 47-year-old woman is brought to the emergency department by her husband with the complaints of severe abdominal pain and discomfort. The pain began 2 days earlier, she describes it as radiating to her back and is associated with nausea. Her past medical history is significant for similar episodes of pain after fatty meals that resolved on its own. She drinks socially and has a 15 pack-year smoking history. Her pulse is 121/min, blood pressure is 121/71 mm Hg, and her temperature is 103.1°F (39.5°C). She has tenderness in the right upper quadrant and epigastrium with guarding and rebound tenderness. Bowel sounds are hypoactive. Part of a CBC is given below. What is the next best step in the management of this patient? Hb%: 11 gm/dL Total count (WBC): 13,400/mm3 Differential count: Neutrophils: 80% Lymphocytes: 15% Monocytes: 5% ESR: 45 mm/hr C-reactive protein: 9.9 mg/dL (Normal < 3.0 mg/dL)
A 56-year-old man presents to the emergency department with severe epigastric pain that began an hour prior to presentation. He describes the pain as sharp, 10/10 in severity, and radiating to the back. Swallowing worsens the pain and causes him to cough. Before the pain started, he had been vomiting multiple times per day for the past week. The emesis was yellow and he denied ever seeing blood. Medical history is significant for poorly controlled hypertension, type II diabetes, alcohol use disorder, and 2 prior hospitalizations for acute pancreatitis. He smokes 1 pack of cigarettes per day for the last 35 years, denies illicit drug use, and drinks 3 pints of vodka per day. On physical exam, there is mediastinal crackling in synchrony with cardiac contraction on cardiac auscultation in the left lateral decubitus position. Laboratory testing is significant for leukocytosis. Which of the following is most likely the cause of this patient’s symptoms?
A 32-year-old man and his wife are sent to a fertility specialist after trying to conceive for several years without success. They have had unprotected sex several times a week. He has no history of a serious illness and does not take any medications. There are no concerns about his libido or erections. His female partner is not on contraceptive medication and has a child from a previous marriage. At the clinic, his vitals are normal. Examination of the scrotum on the right side is normal, but on the left side there are many deep and superficial ducts or vessels that feels like a bag of worms on palpation. The lesion is more apparent when the patient bears down. Semen analysis shows a low sperm count with poor motility and an increased percentage of abnormal sperms. Which of the following is the most appropriate next step in management?
A 48-year-old woman with a known past medical history significant for hypertension presents for a second opinion of a left breast lesion. The lesion was characterized as eczema by the patient's primary care physician and improved briefly after a trial of topical steroids. However, the patient is concerned that the lesion has started to grow. On physical examination, there is an erythematous, scaly lesion involving the left breast nipple-areolar complex with weeping drainage. What is the next step in the patient's management?
A 37-year-old woman is brought to the emergency department 15 minutes after falling down a flight of stairs. On arrival, she has shortness of breath, right-sided chest pain, right upper quadrant abdominal pain, and right shoulder pain. She is otherwise healthy. She takes no medications. She appears pale. Her temperature is 37°C (98.6°F), pulse is 115/min, respirations are 20/min, and blood pressure is 85/45 mm Hg. Examination shows several ecchymoses over the right chest. There is tenderness to palpation over the right chest wall and right upper quadrant of the abdomen. Bowel sounds are normal. Cardiopulmonary examination shows no abnormalities. Neck veins are flat. Which of the following is the most likely diagnosis?
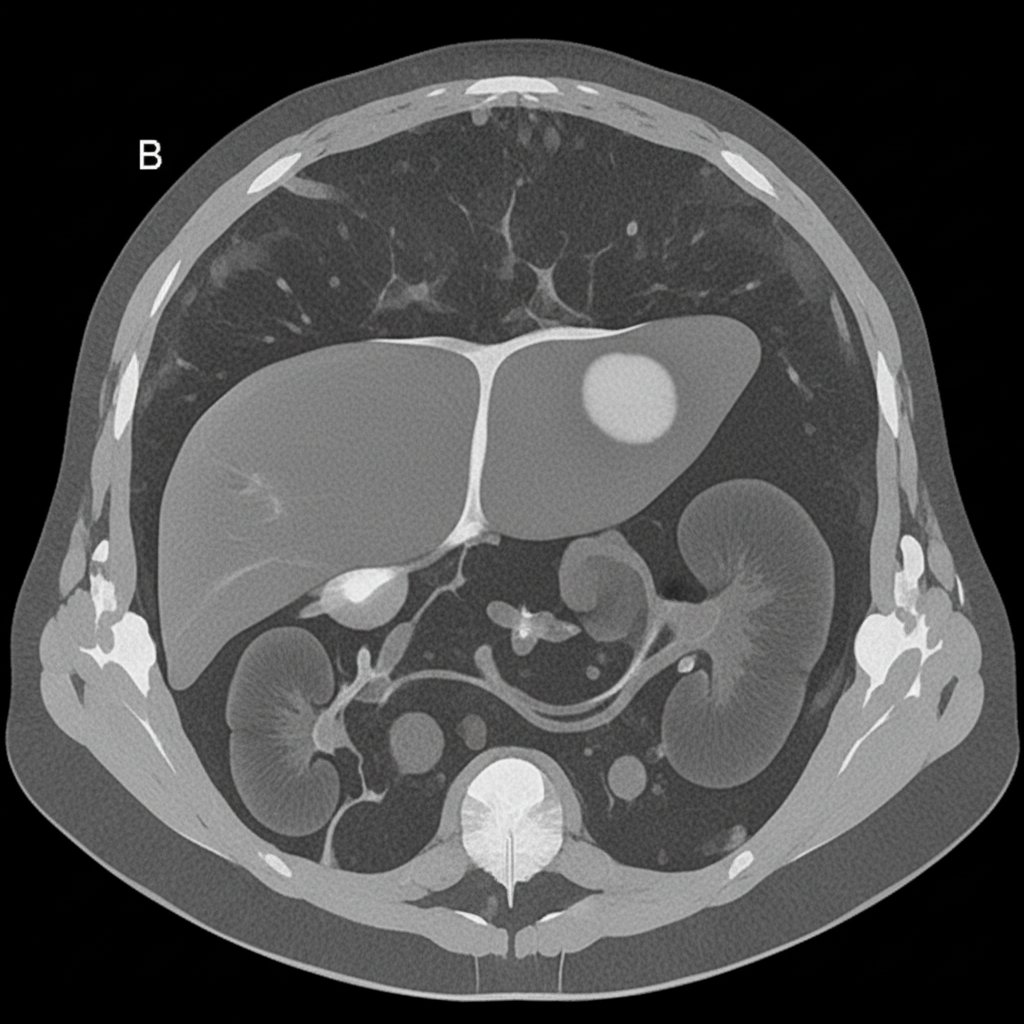
A 27-year-old woman presents with acute abdominal pain in her right upper quadrant. The pain came on suddenly while she was eating dinner. After this pain she began feeling dizzy and came to the emergency department. In the ED, her blood pressure is 75/40 mmHg, pulse is 100/minute, and she is afebrile. On physical exam, she feels too light-headed to ambulate. She demonstrates normal bowel sounds with tenderness upon palpation in the right upper quadrant. The patient is deemed too unstable for imaging. A CT is reviewed from a recent previous visit to the ED for mild abdominal pain, and is shown in Figure B. Which of the following specific additional findings in her history supports the most likely diagnosis?
Practice by Chapter
Acute appendicitis
Practice Questions
Acute cholecystitis
Practice Questions
Small bowel obstruction
Practice Questions
Large bowel obstruction
Practice Questions
Mesenteric ischemia
Practice Questions
Gastrointestinal perforation
Practice Questions
Abdominal compartment syndrome
Practice Questions
Acute pancreatitis management
Practice Questions
Diverticulitis
Practice Questions
Incarcerated/strangulated hernias
Practice Questions
Non-operative management principles
Practice Questions
Diagnostic approach to acute abdomen
Practice Questions
Damage control surgery
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app