
Abdominal emergencies — MCQs

On this page
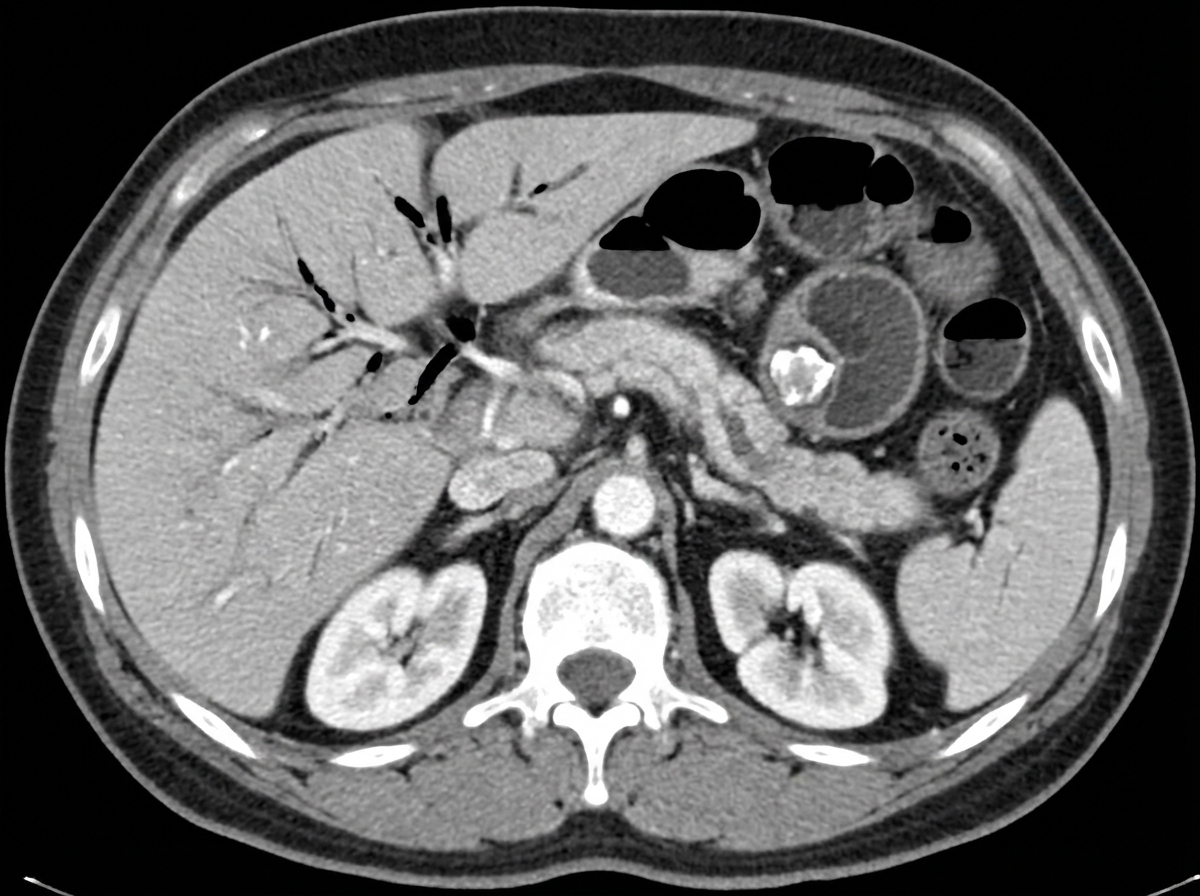
A 67-year-old man comes to the emergency department complaining of severe abdominal pain for the last several hours. The pain is cramp-like in nature, constant, 8/10, and has worsened over time. It is associated with bilious vomiting. He gives a history of episodic right upper abdominal pain for the past few months, mostly after consuming fatty foods, radiating to the tip of the right scapula. He reports no change in bowel habits, bladder habits, or change in weight. His past medical history includes diabetes and hypertension, and he takes hydrochlorothiazide, metformin, ramipril, and atorvastatin. Temperature is 38.2°C (100.8°F), blood pressure is 110/70 mm Hg, pulse is 102/min, respiratory rate is 20/min, and BMI is 23 kg/m2. On physical examination, his abdomen is distended and diffusely tender. Laboratory test Complete blood count Hemoglobin 13 g/dL WBC 16,000/mm3 Platelets 150,000/mm3 Basic metabolic panel Serum Na+ 148 mEq/L Serum K+ 3.3 mEq/L Serum Cl- 89 mEq/L An abdominal CT scan is shown. What is the most likely underlying cause of this patient’s current presentation?
A 47-year-old woman comes to the emergency department 4 hours after the onset of abdominal and right shoulder pain. She has nausea and has had 2 episodes of vomiting. The pain began after her last meal, is constant, and she describes it as 7 out of 10 in intensity. She has had multiple similar episodes over the past 4 months that resolved spontaneously. She drinks 2 pints of vodka daily. She appears ill. Her temperature is 38.4°C (101.1°F), pulse is 110/min, respirations are 20/min, and blood pressure is 165/90 mm Hg. She is alert and fully oriented. Examination shows diaphoresis and multiple telangiectasias over the trunk and back. The abdomen is distended; there is tenderness to palpation in the right upper quadrant. When the patient is asked to inhale with the examiner's hand below the costal margin in the right midclavicular line, the patient winces and her breath catches. Voluntary guarding and shifting dullness are present. The liver is palpated 3 cm below the right costal margin. Laboratory studies show: Hemoglobin 11.5 g/dL Leukocyte count 16,300/mm3 Platelet count 150,000/mm3 Prothrombin time 20 sec (INR=1.3) Serum Urea nitrogen 16 mg/dL Glucose 185 mg/dL Creatinine 1.2 mg/dL Bilirubin (total) 2.1 mg/dL Albumin 3.1 g/dL An abdominal ultrasound shows multiple small stones in the gallbladder and fluid in the gallbladder wall with wall thickening and pericholecystic fluid and stranding. Which of the following is the most appropriate next step in management?
A 48-year-old woman presents with severe chest pain for 2 hours. An episode of severe retching and bloody vomiting preceded the onset of chest pain. She says she had an episode of binge drinking last night. Past medical history includes a gastric ulcer 5 years ago, status post-surgical repair. Her blood pressure is 110/68 mm Hg, pulse is 90/min, respiratory rate is 18/min, and oxygen saturation is 90% on room air. ECG is unremarkable. Her cardiovascular examination is normal. Crepitus is heard over the left lower lobe of the lung. Which of the following is the most likely etiology of this patient’s symptoms?
A 64-year-old man presents to the outpatient clinic because of abdominal pain. He reports that for the last few months, he has had postprandial pain that is worsened by spicy foods. He states that the pain is often located in the right upper portion of his abdomen and feels like it's traveling to his shoulder blade. These episodes are sporadic and unpredictable. He denies any fevers. Physical examination shows no abnormalities. Abdominal ultrasound is shown. Which of the following is the best treatment for this condition?

A 41-year-old woman comes to the physician because of an 8-hour history of colicky abdominal pain and nausea. The pain worsened after she ate a sandwich, and she has vomited once. She has no history of serious medical illness. Her temperature is 37.2°C (99.1°F), pulse is 80/min, and blood pressure is 134/83 mm Hg. Physical examination shows scleral icterus and diffuse tenderness in the upper abdomen. Serum studies show: Total bilirubin 2.7 mg/dL AST 35 U/L ALT 38 U/L Alkaline phosphatase 180 U/L γ-Glutamyltransferase 90 U/L (N = 5–50) Ultrasonography is most likely to show a stone located in which of the following structures?
A 56-year-old man comes to the physician because of intense anal pain that began 2 hours ago. He has a history of chronic constipation and rectal itching. His past medical history is otherwise unremarkable. He takes no medications. His vital signs are within normal limits. Because of extreme pain, a rectal examination is performed in the office under local anesthesia and shows a palpable perianal mass. No skin tag or mucosal prolapse through the anal canal is noted. Which of the following is the most appropriate immediate management?
A 60-year-old woman comes to the physician because of intermittent abdominal pain for the past month. The patient reports that the pain is located in the right upper abdomen and that it does not change with food intake. She has had no nausea, vomiting, or change in weight. She has a history of hypertension and hyperlipidemia. She does not smoke. She drinks 1–2 glasses of wine per day. Current medications include captopril and atorvastatin. Physical examination shows a small, firm mass in the right upper quadrant. Laboratory studies are within the reference range. A CT scan of the abdomen is shown. This patient's condition puts her at increased risk of developing which of the following?

After 1 week of intubation and sedation in the ICU for severe pneumonia, a 62-year-old man develops severe pain in his penis. He has a history of chronic obstructive pulmonary disease. He is an ex-smoker. He is currently on broad-spectrum IV antibiotics. In the ICU, his temperature is 36.7°C (98.1°F), blood pressure is 115/70 mm/Hg, and pulse is 84/min. He is on 2 L of oxygen via nasal cannula and with a respiratory rate of 18/min. On examination, he is uncircumcised with a urinary catheter in place. The foreskin is retracted revealing a severely edematous and erythematous glans. The area is markedly tender to touch. There are no ulcers on the penis or discharge from the urethral meatus. Examination of the scrotum and perineum shows no abnormalities. Which of the following is the most appropriate next step in management?
A 54-year-old woman comes to the physician because of a 6-month history of dull, persistent pain and swelling of her right leg. The pain is worse at the end of the day and is relieved by walking or elevating her feet. Two years ago, she developed acute deep vein thrombosis in her right calf after a long flight, which was treated with anticoagulants for 6 months. Physical examination shows 2+ pitting edema of her right leg. The skin around the right ankle shows a reddish-brown discoloration and multiple telangiectasias. She has dilated varicose veins in the right leg. Which of the following is most likely to establish the diagnosis?
Three days after undergoing coronary artery bypass surgery, a 72-year-old man has severe right upper quadrant pain, fever, nausea, and vomiting. He has type 2 diabetes mellitus, benign prostatic hyperplasia, peripheral vascular disease, and chronic mesenteric ischemia. He had smoked one pack of cigarettes daily for 30 years but quit 10 years ago. He drinks 8 cans of beer a week. His preoperative medications include metformin, aspirin, simvastatin, and finasteride. His temperature is 38.9°C (102°F), pulse is 102/min, respirations are 18/min, and blood pressure is 110/60 mmHg. Auscultation of the lungs shows bilateral inspiratory crackles. Cardiac examination shows no murmurs, rubs or gallops. Abdominal examination shows soft abdomen with tenderness and sudden inspiratory arrest upon palpation in the right upper quadrant. There is no rebound tenderness or guarding. Laboratory studies show the following: Hemoglobin 13.1 g/dL Hematocrit 42% Leukocyte count 15,700/mm3 Segmented neutrophils 65% Bands 10% Lymphocytes 20% Monocytes 3% Eosinophils 1% Basophils 0.5% AST 40 U/L ALT 100 U/L Alkaline phosphatase 85 U/L Total bilirubin 1.5 mg/dL Direct 0.9 mg/dL Amylase 90 U/L Abdominal ultrasonography shows a distended gallbladder, thickened gallbladder wall with pericholecystic fluid, and no stones. Which of the following is the most appropriate next step in management?
Practice by Chapter
Acute appendicitis
Practice Questions
Acute cholecystitis
Practice Questions
Small bowel obstruction
Practice Questions
Large bowel obstruction
Practice Questions
Mesenteric ischemia
Practice Questions
Gastrointestinal perforation
Practice Questions
Abdominal compartment syndrome
Practice Questions
Acute pancreatitis management
Practice Questions
Diverticulitis
Practice Questions
Incarcerated/strangulated hernias
Practice Questions
Non-operative management principles
Practice Questions
Diagnostic approach to acute abdomen
Practice Questions
Damage control surgery
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app