
Abdominal emergencies — MCQs

On this page
A 54-year-old woman comes to the emergency department because of a 5-hour history of diffuse, severe abdominal pain, nausea, and vomiting. She reports that there is no blood or bile in the vomitus. Two weeks ago, she started having mild aching epigastric pain, which improved with eating. Since then, she has gained 1.4 kg (3 lb). She has a 2-year history of osteoarthritis of both knees, for which she takes ibuprofen. She drinks 1–2 glasses of wine daily. She is lying supine with her knees drawn up and avoids any movement. Her temperature is 38.5°C (101.3°F), pulse is 112/min, respirations are 20/min, and blood pressure is 115/70 mm Hg. Physical examination shows abdominal tenderness and guarding; bowel sounds are decreased. An x-ray of the chest is shown. Which of the following is the most likely cause of this patient's current symptoms?

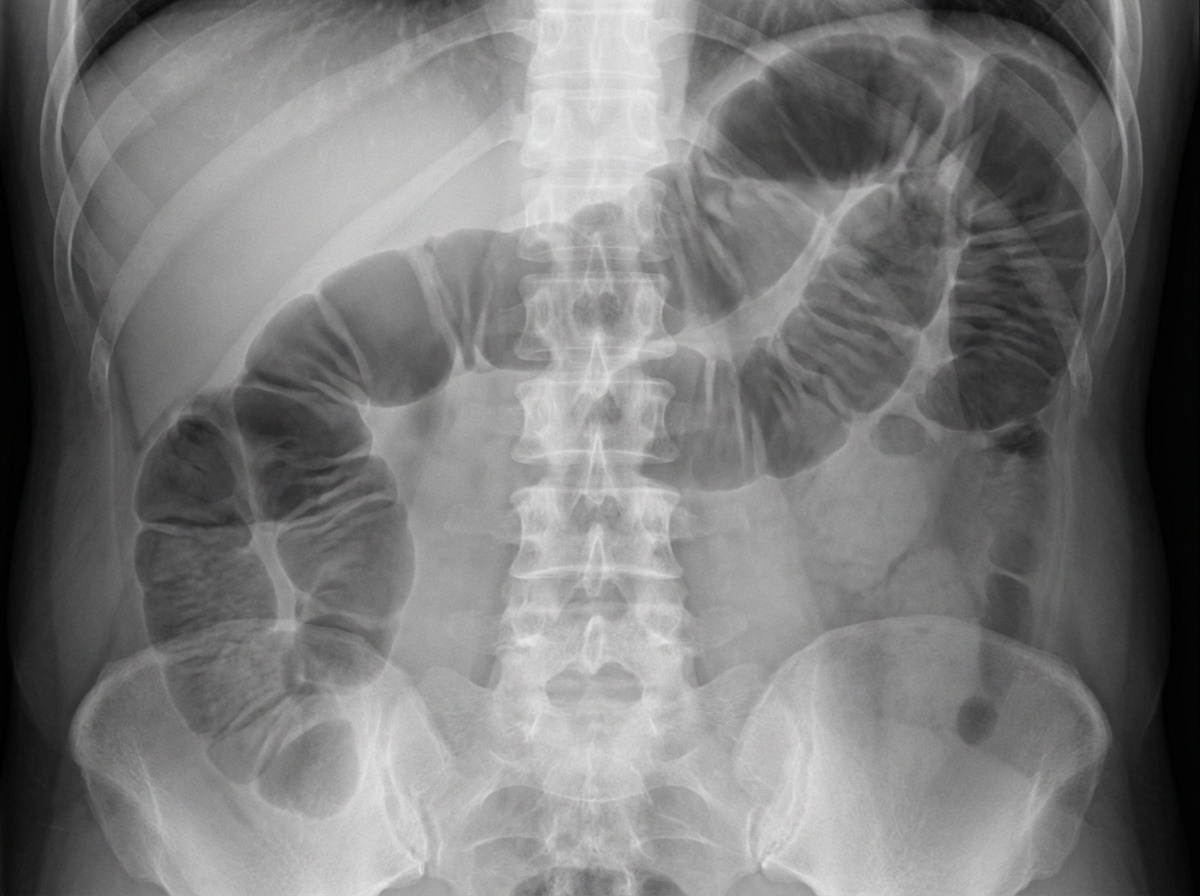
A 63-year-old man is brought to the emergency department for evaluation of abdominal pain. The pain started four days ago and is now a diffuse crampy pain with an intensity of 6/10. The patient has nausea and has vomited twice today. His last bowel movement was three days ago. He has a history of hypertension and recurrent constipation. Five years ago, he underwent emergency laparotomy for a perforated duodenal ulcer. His father died of colorectal cancer at the age of 65 years. The patient has been smoking one pack of cigarettes daily for the past 40 years. Current medications include lisinopril and lactulose. His temperature is 37.6°C (99.7°F), pulse is 89/min, and blood pressure is 120/80 mm Hg. Abdominal examination shows distention and mild tenderness to palpation. There is no guarding or rebound tenderness. The bowel sounds are high-pitched. Digital rectal examination shows no abnormalities. An x-ray of the abdomen is shown. In addition to fluid resuscitation, which of the following is the most appropriate next step in the management of this patient?
A 67-year-old man presents to the emergency department with abdominal pain that started 1 hour ago. The patient has a past medical history of diabetes and hypertension as well as a 40 pack-year smoking history. His blood pressure is 107/58 mmHg, pulse is 130/min, respirations are 23/min, and oxygen saturation is 98% on room air. An abdominal ultrasound demonstrates focal dilation of the aorta with peri-aortic fluid. Which of the following is the best next step in management?
A 61-year-old man comes to the physician because of several episodes of dark urine over the past 2 weeks. He does not have dysuria or flank pain. He works in a factory that produces dyes. Since an accident at work 5 years ago, he has had moderate hearing loss bilaterally. He takes no medications. He has smoked a pack of cigarettes daily for 29 years and drinks one alcoholic beverage daily. Vital signs are within normal limits. Physical examination shows no abnormalities. His urine is pink; urinalysis shows 80 RBC/hpf but no WBCs. Cystoscopy shows a 3-cm mass in the bladder mucosa. The mass is resected. Pathologic examination shows an urothelial carcinoma with penetration into the muscular layer. An x-ray of the chest and a CT scan of the abdomen and pelvis with contrast show a normal upper urinary tract and normal lymph nodes. Which of the following is the most appropriate next step in management?
A 5-week-old infant boy presents to the pediatrician with intermittent vomiting for the last 2 weeks. The mother reports that the vomiting is non-bilious and immediately follows feeding. After vomiting, the baby is hungry and wants to feed again. The frequency of vomiting has been increasing progressively over 2 weeks. The vital signs are within normal limits. The examination of the abdomen reveals the presence of a firm mass of approx. 2 cm in length, above and to the right of the umbilicus. The mass is movable, olive-shaped, and hard on palpation. Which of the following is the most likely surgical treatment for this infant’s condition?
A 67-year-old woman is brought to the emergency department by her husband because of a 1-hour history of severe groin pain, nausea, and vomiting. She has had a groin swelling that worsens with standing, coughing, and straining for the past 3 months. Her pulse is 120/min. Examination shows pallor; there is swelling, erythema, and tenderness to palpation of the right groin that is centered below the inguinal ligament. The most likely cause of this patient's condition is entrapment of an organ between which of the following structures?
A 75-year-old man presents to the emergency department for abdominal pain. The patient states the pain started this morning and has been worsening steadily. He decided to come to the emergency department when he began vomiting. The patient has a past medical history of obesity, diabetes, alcohol abuse, and hypertension. His current medications include captopril, insulin, metformin, sodium docusate, and ibuprofen. His temperature is 104.0°F (40°C), blood pressure is 160/97 mmHg, pulse is 90/min, respirations are 15/min, and oxygen saturation is 98% on room air. Abdominal exam reveals left lower quadrant tenderness. Cardiac exam reveals a crescendo systolic murmur heard best by the right upper sternal border. Lab values are ordered and return as below. Hemoglobin: 15 g/dL Hematocrit: 42% Leukocyte count: 19,500 cells/mm^3 with normal differential Platelet count: 226,000/mm^3 Serum: Na+: 139 mEq/L Cl-: 101 mEq/L K+: 4.4 mEq/L HCO3-: 24 mEq/L BUN: 22 mg/dL Glucose: 144 mg/dL Creatinine: 1.2 mg/dL Ca2+: 9.8 mg/dL Which of the following is the most accurate test for this patient's condition?
A 67-year-old man presents to his primary care provider with bloody urine. He first noticed the blood 1 week ago. He otherwise feels healthy. His past medical history is significant for type 2 diabetes mellitus for 18 years, for which he takes insulin injections. He has smoked 30–40 cigarettes per day for the past 29 years and drinks alcohol socially. Today his vital signs include: temperature 36.6°C (97.8°F), blood pressure 135/82 mm Hg, and heart rate 105/min. There are no findings on physical examination. Urinalysis shows 15–20 red cells/high power field. Which of the following is the next best test to evaluate this patient’s condition?
A 74-year-old man is brought to the emergency department because of lower abdominal pain for 3 hours. The pain is sharp, constant, and does not radiate. He has not urinated for 24 hours and he has not passed stool for over 3 days. He was diagnosed with herpes zoster 3 weeks ago and has been taking amitriptyline for post-herpetic neuralgia for 1 week. Last year he was diagnosed with nephrolithiasis and was treated with lithotripsy. He has a history of hypertension, benign prostatic hyperplasia, and coronary artery disease. His other medications include amlodipine, metoprolol, tamsulosin, aspirin, and simvastatin. He appears uncomfortable. His temperature is 37.3°C (99.1°F), pulse is 102/min, and blood pressure is 140/90 mm Hg. Abdominal examination shows a palpable lower midline abdominal mass that is tender to palpation. Bowel sounds are hypoactive. The remainder of the examination shows no abnormalities. A pelvic ultrasound shows an anechoic mass in the lower abdomen. Which of the following is the most appropriate next step in the management of this patient?
A 75-year-old Caucasian man presents to the emergency department with abdominal pain. The patient states he was at home eating dinner when he began to experience severe abdominal pain. The patient has a past medical history of diabetes, hypertension, and atherosclerosis. He lives at home alone, smokes cigarettes, and drinks 1 to 2 alcoholic drinks per day. The patient is given IV morphine and an ultrasound is obtained demonstrating a dilated abdominal aorta. The patient states that his father died of a similar finding and is concerned about his prognosis. Which of the following is the greatest risk factor for this patient's presentation?
Practice by Chapter
Acute appendicitis
Practice Questions
Acute cholecystitis
Practice Questions
Small bowel obstruction
Practice Questions
Large bowel obstruction
Practice Questions
Mesenteric ischemia
Practice Questions
Gastrointestinal perforation
Practice Questions
Abdominal compartment syndrome
Practice Questions
Acute pancreatitis management
Practice Questions
Diverticulitis
Practice Questions
Incarcerated/strangulated hernias
Practice Questions
Non-operative management principles
Practice Questions
Diagnostic approach to acute abdomen
Practice Questions
Damage control surgery
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app