
Abdominal emergencies — MCQs

On this page
A 40-year-old woman comes to the physician because of a 2-week history of anal pain that occurs during defecation and lasts for several hours. She reports that she often strains during defecation and sees bright red blood on toilet paper after wiping. She typically has 3 bowel movements per week. Physical examination shows a longitudinal, perianal tear. This patient's symptoms are most likely caused by tissue injury in which of the following locations?
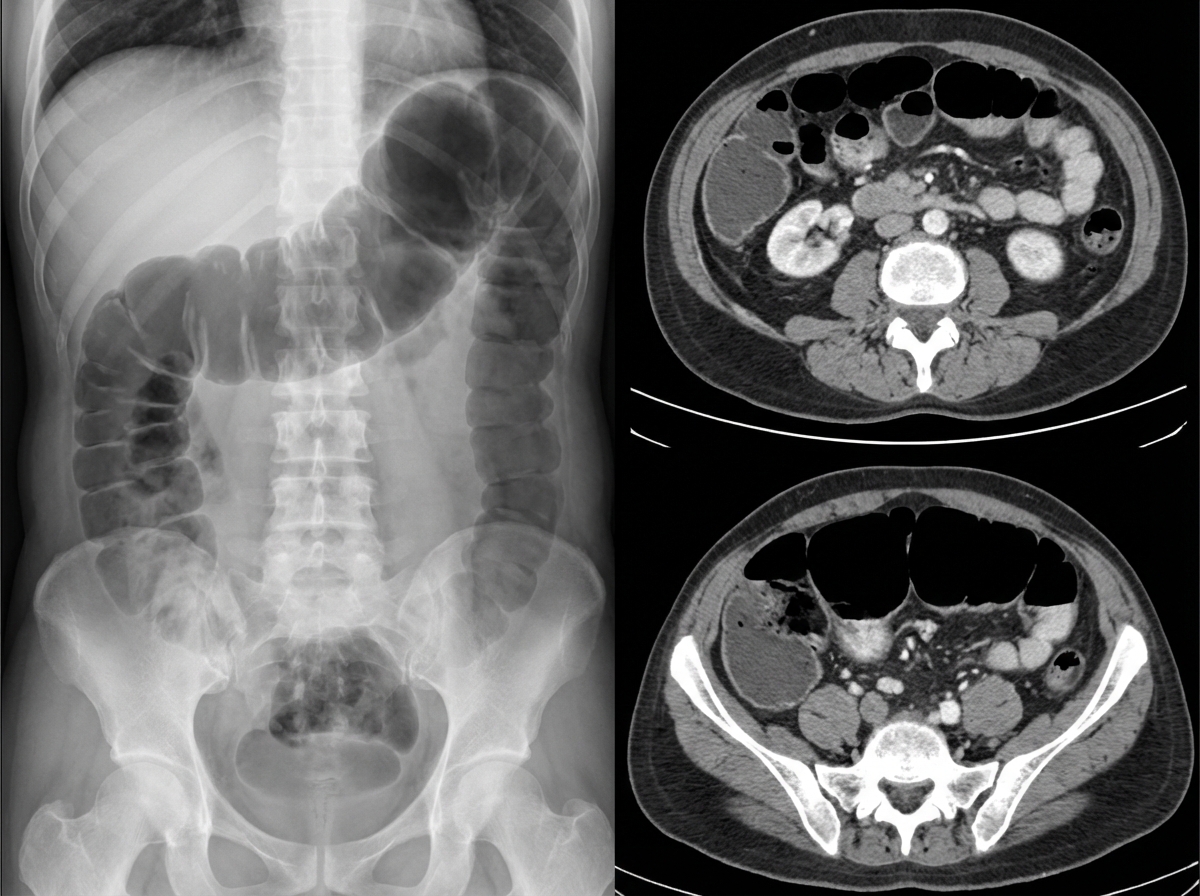
A 76-year-old female is brought to the emergency department after being found unresponsive in her room at her nursing facility. Past medical history is significant for Alzheimer's disease, hypertension, and diabetes. Surgical history is notable for an open cholecystectomy at age 38 and multiple cesarean sections. On arrival, she is non-responsive but breathing by herself, and her vital signs are T 102.9 F, HR 123 bpm, BP 95/64, RR 26/min, and SaO2 97% on 6L nasal cannula. On physical exam the patient has marked abdominal distension and is tympanic to percussion. Laboratory studies are notable for a lactic acidosis. An upright abdominal radiograph and CT abdomen/pelvis with contrast are shown in Figures A and B respectively. She is started on IV fluids and a nasogastric tube is placed to suction which returns green bilious fluid. Repeat vitals 1 hour later are T 101F, HR 140 bpm, BP 75/44, RR 30/min, and SaO2 is 100% on the ventilator after she is intubated for airway concerns. What is the next best step in management?
A 69-year-old man is brought to the emergency department because of severe abdominal pain radiating to his left flank for 30 minutes. He is weak and has been unable to stand since the onset of the pain. He vomited twice on the way to the hospital. He has not passed stools for 3 days. He has hypertension, coronary heart disease, and peptic ulcer disease. He has smoked half a pack of cigarettes daily for 46 years. Current medications include enalapril, metoprolol, aspirin, simvastatin, and pantoprazole. He appears ill. His temperature is 37°C (98.6°F), pulse is 131/min, respirations are 31/min, and blood pressure is 82/56 mm Hg. Pulse oximetry on room air shows an oxygen saturation of 92%. The lungs are clear to auscultation. Cardiac examination shows no abnormalities. Examination shows a painful pulsatile abdominal mass. Intravenous fluid resuscitation is begun. Which of the following is the most appropriate next step in management?
A 31-year-old man presents to an urgent care clinic with symptoms of lower abdominal pain, bloating, bloody diarrhea, and fullness, all of which have become more frequent over the last 3 months. His vital signs are as follows: blood pressure is 121/81 mm Hg, heart rate is 87/min, and respiratory rate is 15/min. Rectal examination reveals a small amount of bright red blood. Lower endoscopy is performed, showing extensive mucosal erythema, induration, and pseudopolyps extending from the rectum to the splenic flexure. Given the following options, what is the most appropriate initial treatment for this patient's underlying disease?
A 60-year-old woman presents with changes in her left breast that started 1 month ago. The patient states that she noticed that an area of her left breast felt thicker than before, and has not improved. She came to get it checked out because her best friend was just diagnosed with invasive ductal carcinoma. The past medical history is significant for Hashimoto’s thyroiditis, well-managed medically with levothyroxine. The patient has a 30-pack-year smoking history, but she quit over 15 years ago. The menarche occurred at age 11, and the menopause was at age 53. She does not have any children and has never been sexually active. Her last screening mammogram 10 months ago was normal. The family history is significant for her mother dying from a myocardial infarction (MI) at age 68, her sister dying from metastatic breast cancer at age 55, and for colon cancer in her paternal grandfather. The review of systems is notable for unintentional weight loss of 3.6 kg (8 lb) in the past month. The vital signs include: temperature 37.0℃ (98.6℉), blood pressure 110/70 mm Hg, pulse 72/min, respiratory rate 15/min, and oxygen saturation 98% on room air. The physical examination is significant only for a minimally palpable mass with irregular, poorly defined margins in the upper outer quadrant of the left breast. The mass is rubbery and movable. There is no axillary lymphadenopathy noted. Which of the following characteristics is associated with this patient’s most likely type of breast cancer in comparison to her friend’s diagnosis?
A 32-year-old man presents to his primary care physician complaining of pain accompanied by a feeling of heaviness in his scrotum. He is otherwise healthy except for a broken arm he obtained while skiing several years ago. Physical exam reveals an enlarged “bag of worms” upon palpation of the painful scrotal region. Shining a light over this area shows that the scrotum does not transilluminate. Which of the following statements is true about the most likely cause of this patient's symptoms?
A 28-year-old man comes to the physician because of a 2-week history of testicular swelling and dull lower abdominal discomfort. Physical examination shows a firm, nontender left testicular nodule. Ultrasonography of the scrotum shows a well-defined hypoechoic lesion of the left testicle. Serum studies show an elevated β-hCG concentration and a normal α-fetoprotein concentration. The patient undergoes a radical inguinal orchiectomy. Histopathologic examination of the surgical specimen shows a mixed germ cell tumor with invasion of adjacent lymphatic vessels. Further evaluation is most likely to show malignant cells in which of the following lymph node regions?
A 23-year-old woman presents to the emergency department with severe abdominal pain. She states that the pain has been dull and progressive, but became suddenly worse while she was exercising. The patient's past medical history is notable for depression, anxiety, and gonococcal urethritis that was appropriately treated. The patient states that she is sexually active and does not use condoms. She admits to drinking at least 5 standard alcoholic drinks a day. The patient also recently lost a large amount of weight for a fitness show she planned on entering. The patient's current medications include oral contraceptive pills, fluoxetine, alprazolam, ibuprofen, acetaminophen, and folate. On physical exam you note an athletic young woman with burly shoulders, a thick neck, and acne on her forehead and back. On abdominal exam you note diffuse tenderness with 10/10 pain upon palpation of the right upper quadrant. Blood pressure is 80/40 mmHg, pulse is 110/minute, temperature is 99.5°F (37.5°C) and respirations are 15/minute with an oxygen saturation of 96% on room air. Intravenous fluids are started and labs are sent. A urinary ß-hCG has been ordered. Which of the following is most likely the diagnosis?
A 2-year-old female with abdominal pain undergoes laparoscopic surgery. An outpouching of tissue is excised from the ileum and sent to the laboratory for evaluation. The pathologist notes inflammation and the presence of mucosa, submucosa, and muscle in the walls of the specimen. Which of the following is the most likely diagnosis?
A 68-year-old male with past history of hypertension, hyperlipidemia, and a 30 pack/year smoking history presents to his primary care physician for his annual physical. Because of his age and past smoking history, he is sent for screening abdominal ultrasound. He is found to have a 4 cm infrarenal abdominal aortic aneurysm. Surgical repair of his aneurysm is indicated if which of the following are present?
Practice by Chapter
Acute appendicitis
Practice Questions
Acute cholecystitis
Practice Questions
Small bowel obstruction
Practice Questions
Large bowel obstruction
Practice Questions
Mesenteric ischemia
Practice Questions
Gastrointestinal perforation
Practice Questions
Abdominal compartment syndrome
Practice Questions
Acute pancreatitis management
Practice Questions
Diverticulitis
Practice Questions
Incarcerated/strangulated hernias
Practice Questions
Non-operative management principles
Practice Questions
Diagnostic approach to acute abdomen
Practice Questions
Damage control surgery
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app