
Large bowel obstruction — MCQs

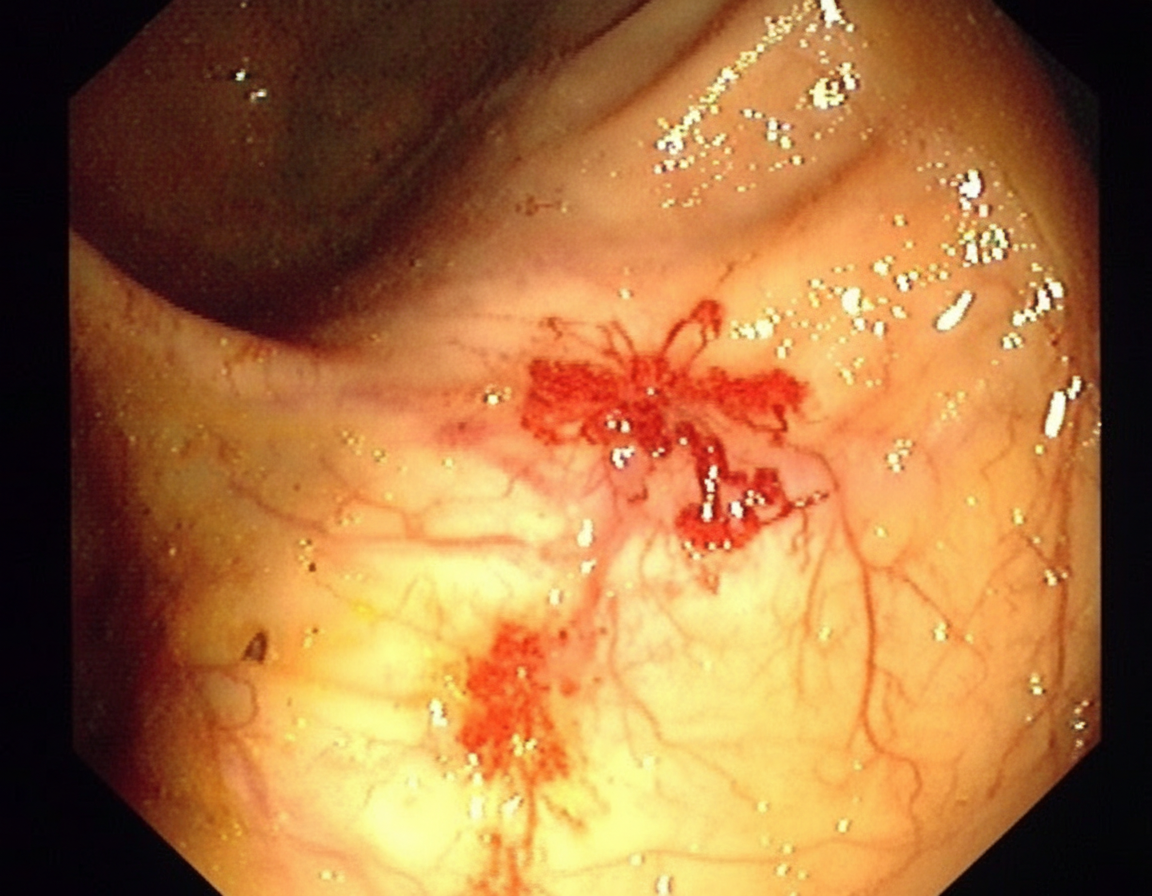
A 70-year-old man comes to the clinic for generalized fatigue. He says that he is more tired than before and has difficulty catching his breath while walking upstairs. He feels tired quickly doing his usual activity such as gardening and shopping. He does not have any symptoms of fever, change in bowel habits, abdominal pain, rectal bleeding, or weight loss. His appetite is normal. His last colonoscopy was done 10 years ago and it was normal. His blood pressure is 116/74 and heart rate is 87/min. On physical examination, his conjunctivae are pale. A routine blood test shows iron deficiency anemia with hemoglobin of 10 gm/dL. His stool is positive for occult blood. He is then sent for a colonoscopy (image is shown). What is the most likely diagnosis for the above condition?
A 60-year-old patient presents to the urgent care clinic with complaints of pain and abdominal distention for the past several weeks. The pain began with a change in bowel habits 3 months ago, and he gradually defecated less until he became completely constipated, which led to increasing pain and distention. He also mentions that he has lost weight during this period, even though he has not changed his diet. When asked about his family history, the patient reveals that his brother was diagnosed with colorectal cancer at 65 years of age. An abdominal radiograph and CT scan were done which confirmed the diagnosis of obstruction. Which of the following locations in the digestive tract are most likely involved in this patient’s disease process?
A 68-year-old woman is brought to the emergency department with intense abdominal pain for the past 2 hours. She has had 1 episode of bloody diarrhea recently. She has an 18-year history of diabetes mellitus. She was diagnosed with hypertension and ischemic heart disease 6 years ago. She is fully alert and oriented. Her temperature is 37.5°C (99.5°F), blood pressure is 145/90 mm Hg, pulse is 78/min, and respirations are 14/min. Abdominal examination shows mild generalized abdominal tenderness without guarding or rebound tenderness. An abdominal plain X-ray shows no abnormalities. Abdominal CT reveals colonic wall thickening and pericolonic fat stranding in the splenic curvature. Bowel rest, intravenous hydration, and IV antibiotics are initiated. Which of the following is the most important diagnostic evaluation at this time?
A 47-year-old woman presents to the emergency department with abdominal pain. The patient states that she felt this pain come on during dinner last night. Since then, she has felt bloated, constipated, and has been vomiting. Her current medications include metformin, insulin, levothyroxine, and ibuprofen. Her temperature is 99.0°F (37.2°C), blood pressure is 139/79 mmHg, pulse is 95/min, respirations are 12/min, and oxygen saturation is 98% on room air. On physical exam, the patient appears uncomfortable. Abdominal exam is notable for hypoactive bowel sounds, abdominal distension, and diffuse tenderness in all four quadrants. Cardiac and pulmonary exams are within normal limits. Which of the following is the best next step in management?
An 82-year-old woman presents with 2 months of foul-smelling, greasy diarrhea. She says that she also has felt very tired recently and has had some associated bloating and flatus. She denies any recent abdominal pain, nausea, melena, hematochezia, or vomiting. She also denies any history of recent travel and states that her home has city water. Which of the following tests would be most appropriate to initially work up the most likely diagnosis in this patient?
A 5-year-old girl is brought to a medical office for evaluation of persistent abdominal pain that has worsened over the past 24 hours. The mother states that the girl often has constipation which has worsened over the last 3 days. The mother denies that the girl has had bloody stools. The girl has not had a bowel movement or passed flatulence in 72 hours. She has vomited 3 times since last night and refuses to eat. She has no significant medical history, including no history of surgeries. On exam, there are no abdominal masses; however, the upper abdomen is distended and tympanic. What is the most likely underlying cause of the girl’s symptoms?
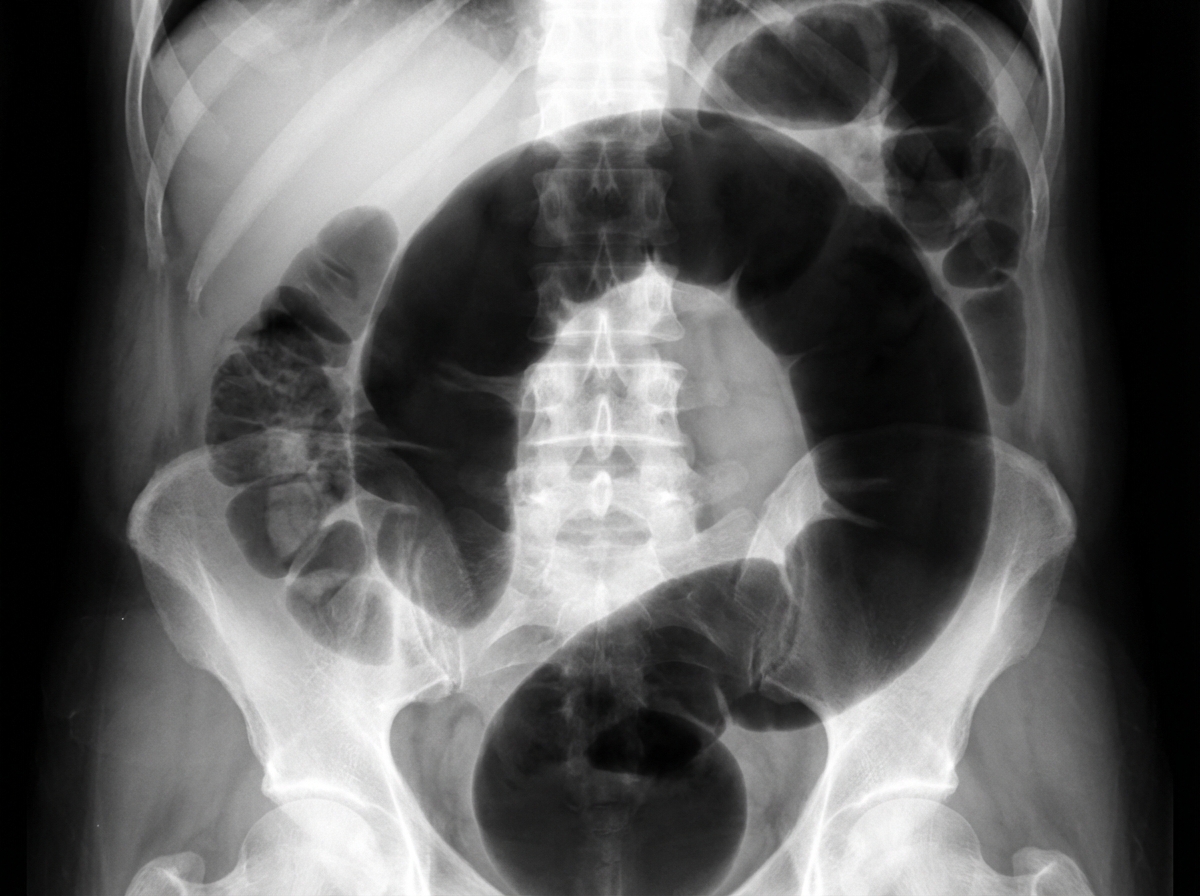
An institutionalized 65-year-old man is brought to the emergency department because of abdominal pain and distension for 12 hours. The pain was acute in onset and is a cramping-type pain associated with nausea, vomiting, and constipation. He has a history of chronic constipation and has used laxatives for years. There is no history of inflammatory bowel disease in his family. He has not been hospitalized recently. There is no recent history of weight loss or change in bowel habits. On physical examination, the patient appears ill. The abdomen is distended with tenderness mainly in the left lower quadrant and is tympanic on percussion. The blood pressure is 110/79 mm Hg, heart rate is 100/min, the respiratory rate is 20/min, and the temperature is 37.2°C (99.0°F). The CBC shows an elevated white blood cell count. The plain abdominal X-ray is shown in the accompanying image. What is the most likely cause of his condition?
A 28-year-old male presents to his primary care physician with complaints of intermittent abdominal pain and alternating bouts of constipation and diarrhea. His medical chart is not significant for any past medical problems or prior surgeries. He is not prescribed any current medications. Which of the following questions would be the most useful next question in eliciting further history from this patient?
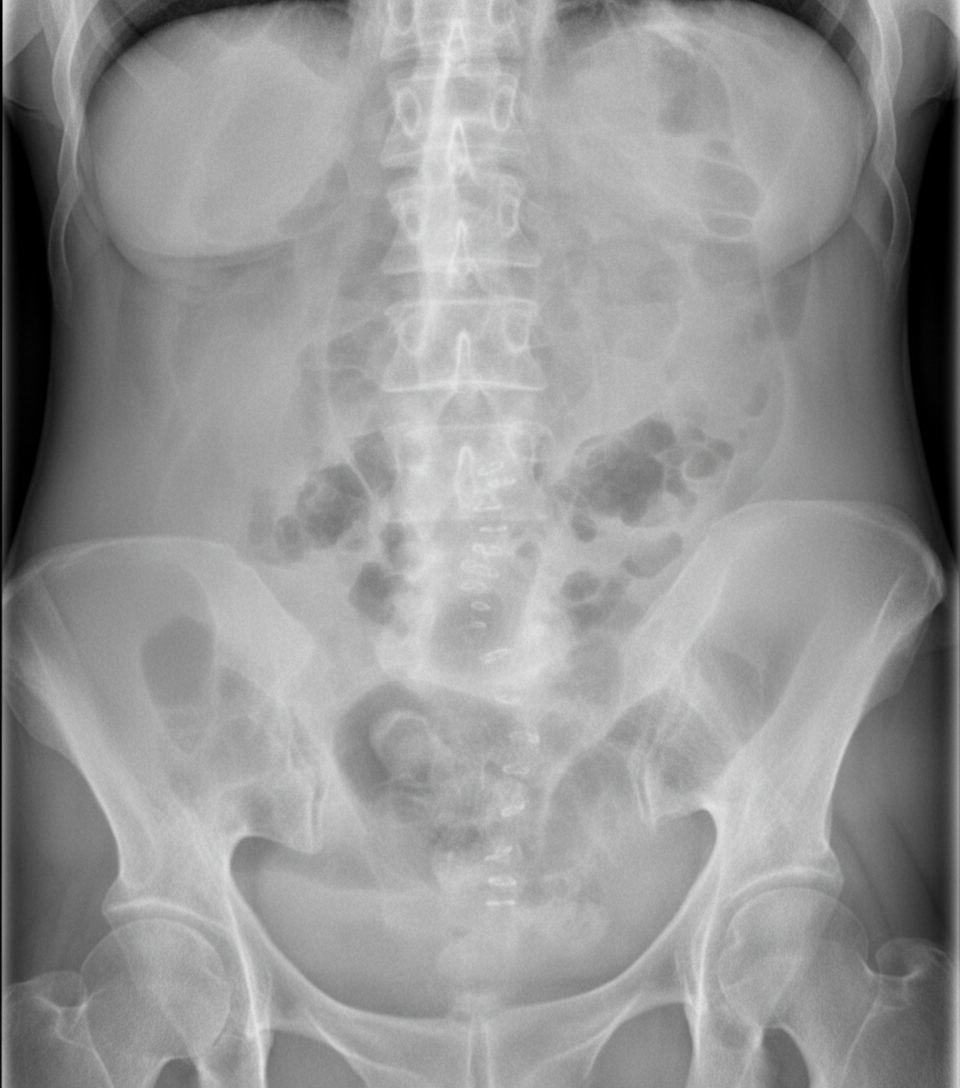
A 75-year-old man is brought to the emergency department after 2 days of severe diffuse abdominal pain, nausea, vomiting, and lack of bowel movements, which has led him to stop eating. He has a history of type-2 diabetes mellitus, hypertension, and chronic obstructive pulmonary disease. Upon admission, his vital signs are within normal limits and physical examination shows diffuse abdominal tenderness, distention, lack of bowel sounds, and an empty rectal ampulla. After initial fluid therapy and correction of moderate hypokalemia, the patient's condition shows mild improvement. His abdominal plain film is taken and shown. Which of the following is the most appropriate concomitant approach?
A 55-year-old man presents to the emergency department with nausea and vomiting. The patient states that he has felt nauseous for the past week and began vomiting last night. He thought his symptoms would resolve but decided to come in when his symptoms worsened. He feels that his symptoms are exacerbated with large fatty meals and when he drinks alcohol. His wife recently returned from a cruise with symptoms of vomiting and diarrhea. The patient has a past medical history of poorly managed diabetes, constipation, anxiety, dyslipidemia, and hypertension. His temperature is 99.5°F (37.5°C), blood pressure is 197/128 mmHg, pulse is 100/min, respirations are 17/min, and oxygen saturation is 95% on room air. Physical exam reveals a systolic murmur heard loudest along the left upper sternal border. Abdominal exam reveals an obese, tympanitic and distended abdomen with a 3 cm scar in the right lower quadrant. Vascular exam reveals weak pulses in the lower extremities. Which of the following is the most likely diagnosis?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app