
Gastrointestinal perforation — MCQs

A 66-year-old man is brought to the emergency department after a motor vehicle accident. The patient was a restrained passenger in a car that was struck on the passenger side while crossing an intersection. In the emergency department, he is alert and complaining of abdominal pain. He has a history of hyperlipidemia, gastroesophageal reflux disease, chronic kidney disease, and perforated appendicitis for which he received an interval appendectomy four years ago. His home medications include rosuvastatin and lansoprazole. His temperature is 99.2°F (37.3°C), blood pressure is 120/87 mmHg, pulse is 96/min, and respirations are 20/min. He has full breath sounds bilaterally. He is tender to palpation over the left 9th rib and the epigastrium. He is moving all four extremities. His FAST exam reveals fluid in Morrison's pouch. This patient is most likely to have which of the following additional signs or symptoms?
A 52-year-old man is brought to the emergency department with severe epigastric discomfort and left-sided chest pain radiating to the back that began after waking up. He has also vomited several times since the pain began. He underwent an esophagogastroduodenoscopy the previous day for evaluation of epigastric pain. He has ischemic heart disease and underwent a coronary angioplasty 3 years ago. His mother died of pancreatic cancer when she was 60 years old. His current medications include aspirin, clopidogrel, metoprolol, ramipril, and rosuvastatin. He is pale, anxious, and diaphoretic. His temperature is 37.9°C (100.2°F), pulse is 140/min, respirations are 20/min, and blood pressure is 100/60 mm Hg in his upper extremities and 108/68 mm Hg in his lower extremities. Pulse oximetry on room air shows oxygen saturation at 98%. An S4 is audible over the precordium, in addition to crepitus over the chest. Abdominal examination shows tenderness to palpation in the epigastric area. Serum studies show an initial Troponin I level of 0.031 ng/mL (N < 0.1 ng/mL) and 0.026 ng/mL 6 hours later. A 12-lead ECG shows sinus tachycardia with nonspecific ST-T changes. Which of the following is the most likely diagnosis?
A 51-year-old man with a recent diagnosis of peptic ulcer disease currently treated with an oral proton pump inhibitor twice daily presents to the urgent care center complaining of acute abdominal pain which began suddenly less than 2 hours ago. On physical exam, you find his abdomen to be mildly distended, diffusely tender to palpation, and positive for rebound tenderness. Given the following options, what is the next best step in patient management?
A 45-year-old man is brought to the emergency department because of severe abdominal pain for the past 2 hours. He has a 2-year history of burning epigastric pain that gets worse with meals. His pulse is 120/min, respirations are 22/min, and blood pressure is 60/40 mm Hg. Despite appropriate lifesaving measures, he dies. At autopsy, examination shows erosion of the right gastric artery. Perforation of an ulcer in which of the following locations most likely caused this patient's findings?
A 52-year-old man comes to the physician because of a 3-month history of upper abdominal pain and nausea that occurs about 3 hours after eating and at night. These symptoms improve with eating. After eating, he often has a feeling of fullness and bloating. He has had several episodes of dark stools over the past month. He has smoked one pack of cigarettes daily for 40 years and drinks 2 alcoholic beverages daily. He takes no medications. His temperature is 36.4°C (97.5°F), pulse is 80/min, and blood pressure is 110/70 mm Hg. Abdominal examination shows epigastric tenderness with no guarding or rebound. Bowel sounds are normal. Which of the following treatments is most appropriate to prevent further complications of the disease in this patient?
A 65-year-old woman presents with severe abdominal pain and bloody diarrhea. Past medical history is significant for a myocardial infarction 6 months ago. The patient reports a 25-pack-year smoking history and consumes 80 ounces of alcohol per week. Physical examination shows a diffusely tender abdomen with the absence of bowel sounds. Plain abdominal radiography is negative for free air under the diaphragm. Laboratory findings show a serum amylase of 115 U/L, serum lipase 95 U/L. Her clinical condition deteriorates rapidly, and she dies. Which of the following would most likely be the finding on autopsy in this patient?
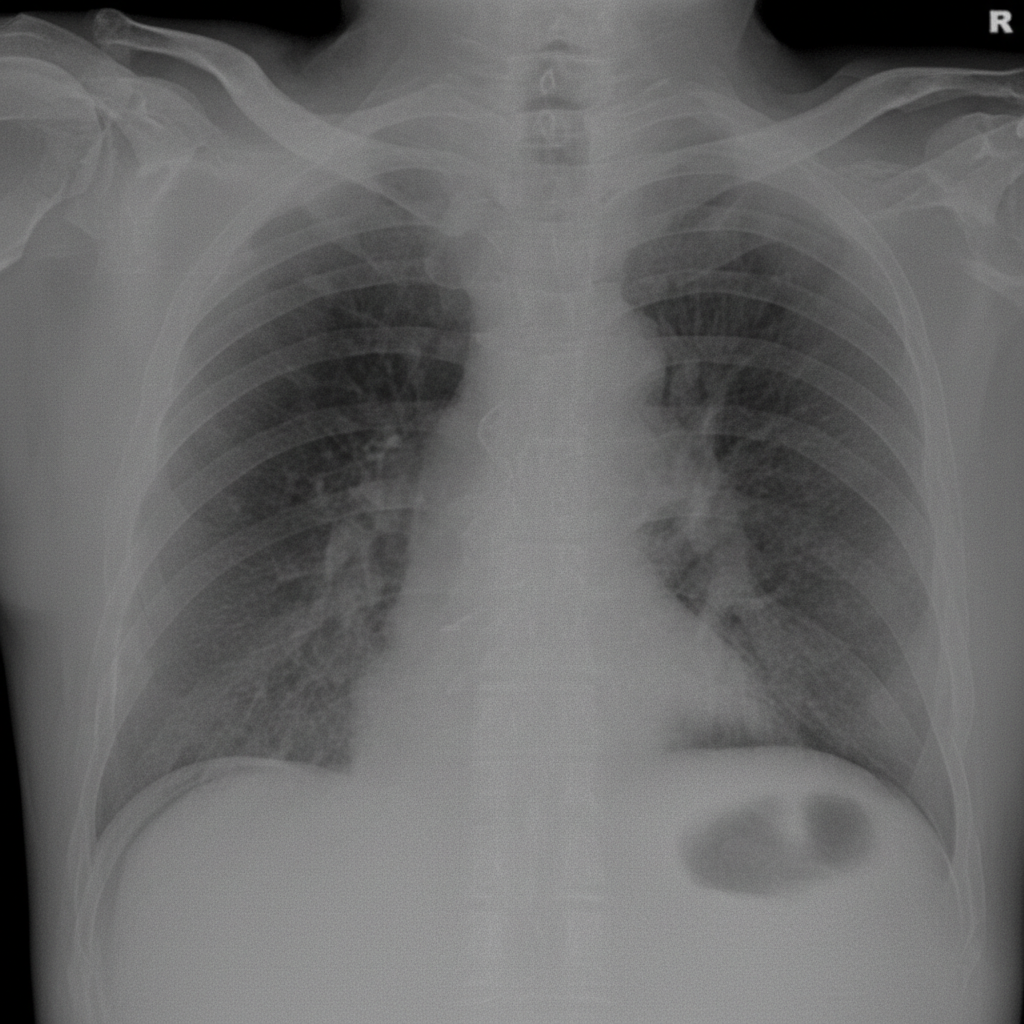
A 56-year-old man is brought to the emergency department after 4 hours of severe abdominal pain with an increase in its intensity over the last hour. His personal history is relevant for peptic ulcer disease and H. pylori infection that is being treated with clarithromycin triple therapy. Upon admission his vital signs are as follows: pulse of 120/min, a respiratory rate of 20/min, body temperature of 39°C (102.2°F), and blood pressure of 90/50 mm Hg. Physical examination reveals significant tenderness over the abdomen. A chest radiograph taken when the patient was standing erect is shown. Which of the following is the next best step in the management of this patient?
A 50-year-old male presents to the emergency with abdominal pain. He reports he has had abdominal pain associated with meals for several months and has been taking over the counter antacids as needed, but experienced significant worsening pain one hour ago in the epigastric region. The patient reports the pain radiating to his shoulders. Vital signs are T 38, HR 120, BP 100/60, RR 18, SpO2 98%. Physical exam reveals diffuse abdominal rigidity with rebound tenderness. Auscultation reveals hypoactive bowel sounds. Which of the following is the next best step in management?
A 68-year-old man presents to the emergency department with left lower quadrant abdominal pain and fever for 1 day. He states during this time frame he has had weight loss and a decreased appetite. The patient had surgery for a ruptured Achilles tendon 1 month ago and is still recovering but is otherwise generally healthy. His temperature is 102°F (38.9°C), blood pressure is 154/94 mmHg, pulse is 90/min, respirations are 15/min, and oxygen saturation is 98% on room air. Physical exam is remarkable for an uncomfortable and thin man with left lower quadrant abdominal tenderness without rebound findings. Fecal occult test for blood is positive. Laboratory studies are ordered as seen below. Hemoglobin: 10 g/dL Hematocrit: 30% Leukocyte count: 3,500/mm^3 with normal differential Platelet count: 157,000/mm^3 Which of the following is the most appropriate next step in management?
A 72-year-old female presents to the emergency department complaining of severe abdominal pain and several days of bloody diarrhea. Her symptoms began with intermittent bloody diarrhea five days ago and have worsened steadily. For the last 24 hours, she has complained of fevers, chills, and abdominal pain. She has a history of ulcerative colitis, idiopathic hypertension, and hypothyroidism. Her medications include hydrochlorothiazide, levothyroxine, and sulfasalazine. In the ED, her temperature is 39.1°C (102.4°F), pulse is 120/min, blood pressure is 90/60 mmHg, and respirations are 20/min. On exam, the patient is alert and oriented to person and place, but does not know the day. Her mucus membranes are dry. Heart and lung exam are not revealing. Her abdomen is distended with marked rebound tenderness. Bowel sounds are hyperactive. Serum: Na+: 142 mEq/L Cl-: 107 mEq/L K+: 3.3 mEq/L HCO3-: 20 mEq/L BUN: 15 mg/dL Glucose: 92 mg/dL Creatinine: 1.2 mg/dL Calcium: 10.1 mg/dL Hemoglobin: 11.2 g/dL Hematocrit: 30% Leukocyte count: 14,600/mm^3 with normal differential Platelet count: 405,000/mm^3 What is the next best step in management?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app