
Diagnostic approach to acute abdomen — MCQs

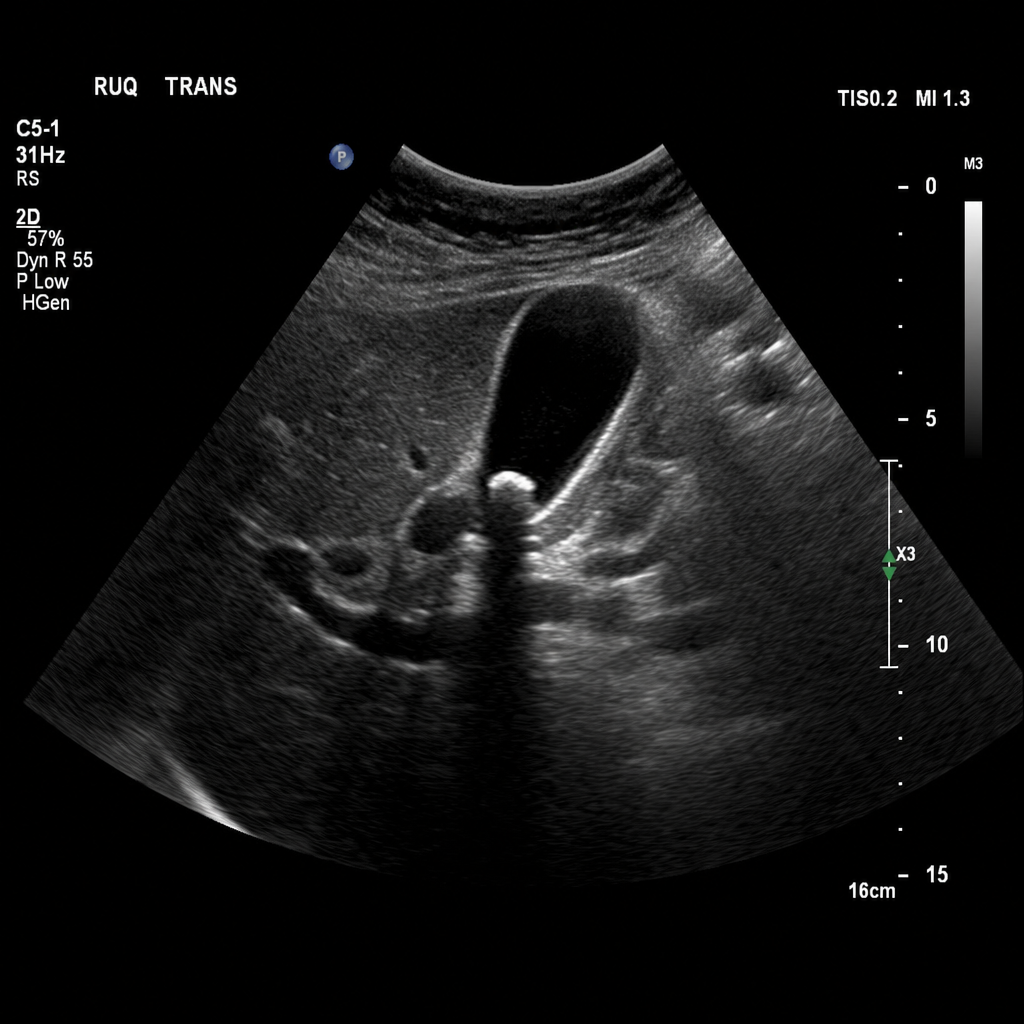
A 43-year-old Caucasian woman is admitted to the hospital with acute onset right upper quadrant (RUQ) pain. The pain started 6 hours ago after the patient had a large meal at a birthday party and has progressively worsened. She recalls having similar pain before but not so intense. No significant past medical history. Current medications are only oral contraceptive. Vitals are blood pressure 140/80 mm Hg, heart rate 79/min, respiratory rate 14/min, and temperature 37.6℃ (99.7℉). The patient’s BMI is 36.3 kg/m2. On exam, the patient appears slightly jaundiced. Her cardiac and respiratory examinations are within normal limits. Abdominal palpation reveals tenderness to palpation in the RUQ with no rebound or guarding, and there is an inspiratory arrest on deep palpation in this region. The remainder of the examination is within normal limits. Laboratory tests are significant for the following: RBC count 4.1 million/mm3 Hb 13.4 mg/dL Leukocyte count 11,200/mm3 ESR 22 mm/hr Platelet count 230,000/mm3 Total bilirubin 2 mg/dL Direct bilirubin 1.1 mg/dL ALT 20 IU/L AST 18 IU/L Amylase 33 IU/L Ultrasound of the abdomen shows the following result (see image): The common bile duct (CBD) (not shown in the image) is not dilated. Which of the following procedures is most appropriate for the treatment of this patient?
A 72-year-old female presents to the emergency department complaining of severe abdominal pain and several days of bloody diarrhea. Her symptoms began with intermittent bloody diarrhea five days ago and have worsened steadily. For the last 24 hours, she has complained of fevers, chills, and abdominal pain. She has a history of ulcerative colitis, idiopathic hypertension, and hypothyroidism. Her medications include hydrochlorothiazide, levothyroxine, and sulfasalazine. In the ED, her temperature is 39.1°C (102.4°F), pulse is 120/min, blood pressure is 90/60 mmHg, and respirations are 20/min. On exam, the patient is alert and oriented to person and place, but does not know the day. Her mucus membranes are dry. Heart and lung exam are not revealing. Her abdomen is distended with marked rebound tenderness. Bowel sounds are hyperactive. Serum: Na+: 142 mEq/L Cl-: 107 mEq/L K+: 3.3 mEq/L HCO3-: 20 mEq/L BUN: 15 mg/dL Glucose: 92 mg/dL Creatinine: 1.2 mg/dL Calcium: 10.1 mg/dL Hemoglobin: 11.2 g/dL Hematocrit: 30% Leukocyte count: 14,600/mm^3 with normal differential Platelet count: 405,000/mm^3 What is the next best step in management?
A 41-year-old woman is brought to the emergency department with the acute-onset of severe abdominal pain for the past 2 hours. She has a history of frequent episodes of vague abdominal pain, but they have never been this severe. Every time she has had pain, it would resolve after eating a meal. Her past medical history is otherwise insignificant. Her vital signs include: blood pressure 121/77 mm Hg, pulse 91/min, respiratory rate 21/min, and temperature 37°C (98.6°F). On examination, her abdomen is flat and rigid. Which of the following is the next best step in evaluating this patient’s discomfort and stomach pain by physical exam?
A 52-year-old woman presents to the urgent care center with several hours of worsening abdominal discomfort with radiation to the back. The patient also complains of malaise, chills, nausea, and vomiting. Social history is notable for alcoholism. On physical exam, she is febrile to 39.5°C (103.1°F), and she is diffusely tender to abdominal palpation. Complete blood count is notable for 13,500 white blood cells, bilirubin 2.1, lipase 842, and amylase 3,210. Given the following options, what is the most likely diagnosis?
A 68-year-old woman is brought to the emergency department with intense abdominal pain for the past 2 hours. She has had 1 episode of bloody diarrhea recently. She has an 18-year history of diabetes mellitus. She was diagnosed with hypertension and ischemic heart disease 6 years ago. She is fully alert and oriented. Her temperature is 37.5°C (99.5°F), blood pressure is 145/90 mm Hg, pulse is 78/min, and respirations are 14/min. Abdominal examination shows mild generalized abdominal tenderness without guarding or rebound tenderness. An abdominal plain X-ray shows no abnormalities. Abdominal CT reveals colonic wall thickening and pericolonic fat stranding in the splenic curvature. Bowel rest, intravenous hydration, and IV antibiotics are initiated. Which of the following is the most important diagnostic evaluation at this time?
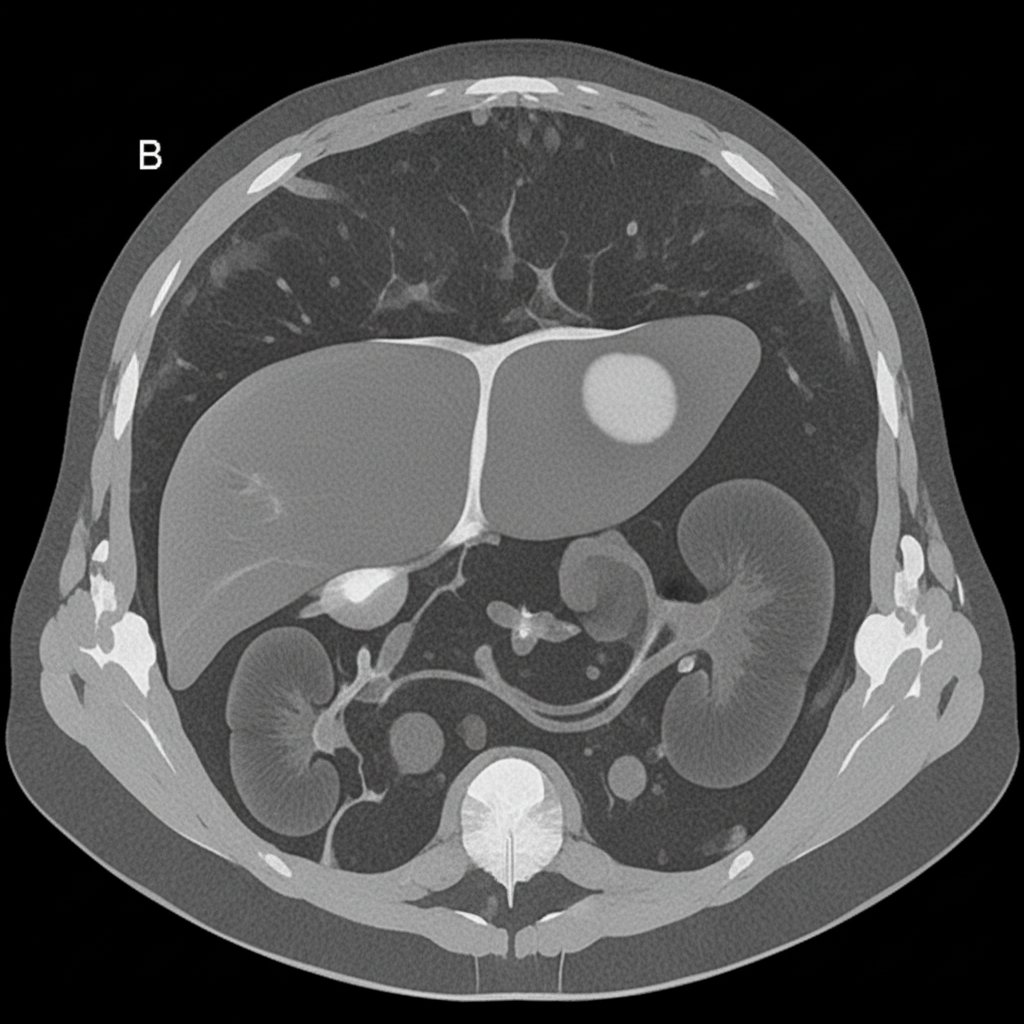
A 27-year-old woman presents with acute abdominal pain in her right upper quadrant. The pain came on suddenly while she was eating dinner. After this pain she began feeling dizzy and came to the emergency department. In the ED, her blood pressure is 75/40 mmHg, pulse is 100/minute, and she is afebrile. On physical exam, she feels too light-headed to ambulate. She demonstrates normal bowel sounds with tenderness upon palpation in the right upper quadrant. The patient is deemed too unstable for imaging. An abdominal radiograph and CT are reviewed from a recent previous visit to the ED for mild abdominal pain, and are shown in Figures A and B, respectively. Which of the following specific additional findings in her history supports the most likely diagnosis?
A 75-year-old man presents to the emergency department for abdominal pain. The patient states the pain started this morning and has been worsening steadily. He decided to come to the emergency department when he began vomiting. The patient has a past medical history of obesity, diabetes, alcohol abuse, and hypertension. His current medications include captopril, insulin, metformin, sodium docusate, and ibuprofen. His temperature is 104.0°F (40°C), blood pressure is 160/97 mmHg, pulse is 90/min, respirations are 15/min, and oxygen saturation is 98% on room air. Abdominal exam reveals left lower quadrant tenderness. Cardiac exam reveals a crescendo systolic murmur heard best by the right upper sternal border. Lab values are ordered and return as below. Hemoglobin: 15 g/dL Hematocrit: 42% Leukocyte count: 19,500 cells/mm^3 with normal differential Platelet count: 226,000/mm^3 Serum: Na+: 139 mEq/L Cl-: 101 mEq/L K+: 4.4 mEq/L HCO3-: 24 mEq/L BUN: 22 mg/dL Glucose: 144 mg/dL Creatinine: 1.2 mg/dL Ca2+: 9.8 mg/dL Which of the following is the most accurate test for this patient's condition?
A 58-year-old man comes to the emergency department with complaints of abdominal pain, swelling, and fever for the last few days. Pain is situated in the right upper quadrant (RUQ) and is dull and aching. He scores it as 6/10 with no exacerbating or relieving factors. He also complains of anorexia for the same duration. The patient experiences a little discomfort while lying flat and has been sleeping in a recliner for the past 2 days. There has been no chest pain, nausea, vomiting, or change in bowel or bladder habit. He does not use tobacco, alcohol, or any recreational drug. He is suffering from polycythemia vera and undergoes therapeutic phlebotomy every 2 weeks, but he has missed several appointments. The patient’s mother died of a heart attack, and his father died from a stroke. Temperature is 38.2°C (100.8°F), blood pressure is 142/88 mm Hg, pulse is 106/min, respirations are 16/min, and BMI is 20 kg/m2. On physical examination, his heart and lungs appear normal. Abdominal exam reveals tenderness to palpation in the RUQ and shifting dullness. Laboratory test Hemoglobin 20.5 g/dL Hematocrit 62% WBC 16,000/mm3 Platelets 250,000/mm3 Albumin 3.8 g/dL Diagnostic paracentesis Albumin 2.2 g/dL WBC 300/µL (reference range: < 500 leukocytes/µL) What is the best next step in management of the patient?
A 42-year-old man presents to the emergency department with abdominal pain. The patient was at home watching television when he experienced sudden and severe abdominal pain that prompted him to instantly call emergency medical services. The patient has a past medical history of obesity, smoking, alcoholism, hypertension, and osteoarthritis. His current medications include lisinopril and ibuprofen. His temperature is 98.5°F (36.9°C), blood pressure is 120/97 mmHg, pulse is 130/min, respirations are 22/min, and oxygen saturation is 97% on room air. The patient is in an antalgic position on the stretcher. His abdomen is rigid and demonstrates rebound tenderness and hypoactive bowel sounds. What is the next best step in management?
A 57-year-old man is admitted to the ER due to an abrupt onset of abdominal pain that radiates to the back, nausea, and multiple vomiting episodes for the past 10 hours. He does not have any significant past medical history. He admits to drinking alcohol every night. During admission, he is found to have a body temperature of 37.5°C (99.5°F), a respiratory rate of 20/min, a pulse of 120/min, and a blood pressure of 120/76 mm Hg. He looks pale with sunken eyes and has significant epigastric tenderness and flank discoloration. An initial laboratory panel shows the following: Total count (WBC) 10,000/mm3 Platelet count 140,000/mm3 Serum glucose 160 mg/dL Serum LDH 500 IU/L Aspartate aminotransferase 400 IU/dL Serum Amylase 500 IU/L Serum Lipase 300 IU/L Which of the following combinations would best predict severity in this case?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app