
Abdominal emergencies — MCQs

On this page
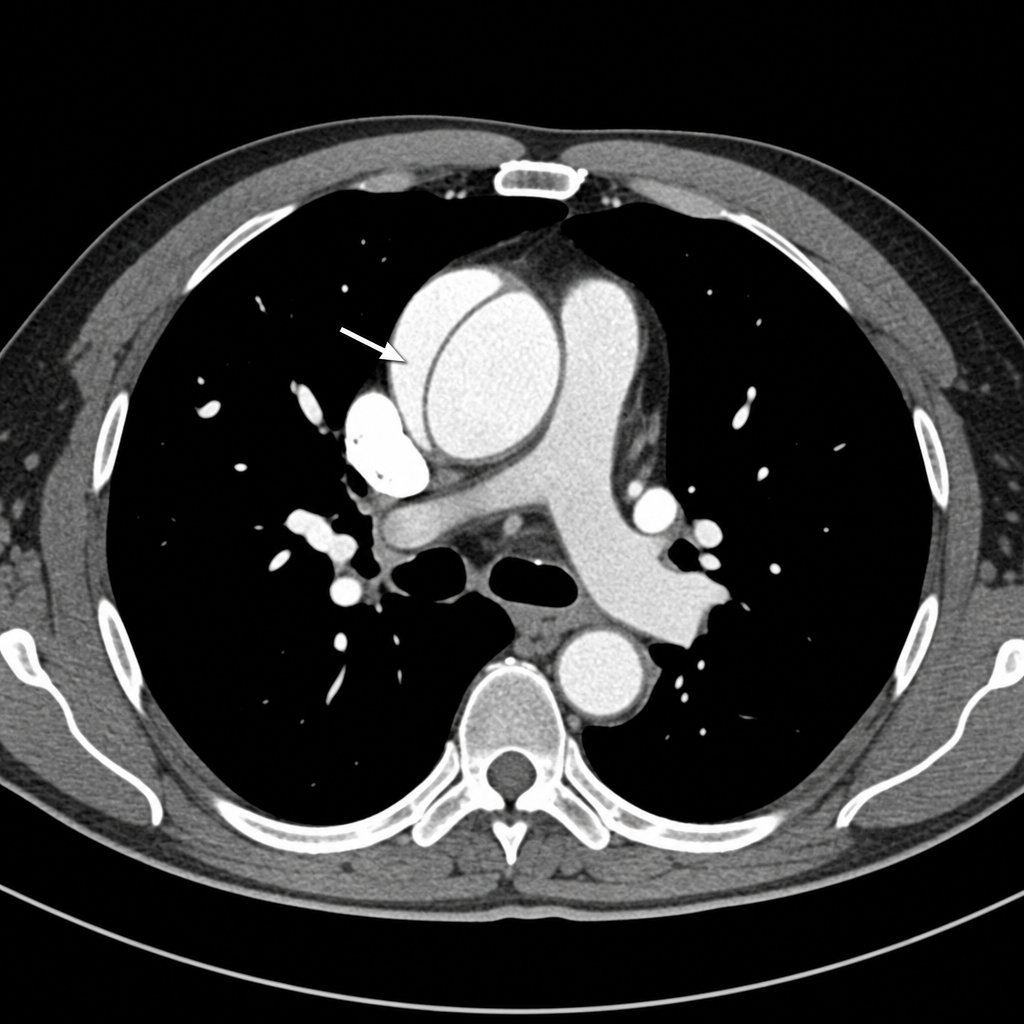
A 67-year-old man with a history of hypertension and a 40-pack-year smoking history presents to the emergency department with sudden-onset tearing chest pain radiating to his back. His blood pressure is 190/100 mmHg in the right arm and 145/85 mmHg in the left arm. A CT scan of the chest with contrast is performed and demonstrates a dissection flap involving the ascending aorta (Stanford Type A). Which of the following is the most appropriate definitive management?
A 24-year-old woman recently noticed a mass in her left breast. The examination shows a 4-cm mass in the left upper quadrant. The mass is firm, mobile, and has well-defined margins. She complains of occasional tenderness. There is no lymphatic involvement. Mammography showed a dense lesion. What is the most likely cause?
A 24-year-old man presents to the emergency department after an altercation at a local bar. The patient was stabbed in the abdomen with a 6 inch kitchen knife in the epigastric region. His temperature is 97°F (36.1°C), blood pressure is 97/68 mmHg, pulse is 127/min, respirations are 19/min, and oxygen saturation is 99% on room air. Physical exam is notable for the knife in the patient’s abdomen in the location where he was initially stabbed. The patient is started on blood products and IV fluids. Which of the following is the best next step in management?
A 79-year-old man presents to the emergency department with abdominal pain. The patient describes the pain as severe, tearing, and radiating to the back. His history is significant for hypertension, hyperlipidemia, intermittent claudication, and a 60 pack-year history of smoking. He also has a previously diagnosed stable abdominal aortic aneurysm followed by ultrasound screening. On exam, the patient's temperature is 98°F (36.7°C), pulse is 113/min, blood pressure is 84/46 mmHg, respirations are 24/min, and oxygen saturation is 99% on room air. The patient is pale and diaphoretic, and becomes confused as you examine him. Which of the following is most appropriate in the evaluation and treatment of this patient?
A 36-year-old woman is brought to the emergency department after the sudden onset of severe, generalized abdominal pain. The pain is constant and she describes it as 9 out of 10 in intensity. She has hypertension, hyperlipidemia, and chronic lower back pain. Menses occur at regular 28-day intervals with moderate flow and last 4 days. Her last menstrual period was 2 weeks ago. She is sexually active with one male partner and uses condoms inconsistently. She has smoked one pack of cigarettes daily for 15 years and drinks 2–3 beers on the weekends. Current medications include ranitidine, hydrochlorothiazide, atorvastatin, and ibuprofen. The patient appears ill and does not want to move. Her temperature is 38.4°C (101.1°F), pulse is 125/min, respirations are 30/min, and blood pressure is 85/40 mm Hg. Examination shows a distended, tympanic abdomen with diffuse tenderness, guarding, and rebound; bowel sounds are absent. Her leukocyte count is 14,000/mm3 and hematocrit is 32%. Which of the following is the most likely cause of this patient's pain?
A 39-year-old woman presents to the emergency department with right upper quadrant abdominal discomfort for the past couple of hours. She says that the pain is dull in nature and denies any radiation. She admits to having similar episodes of pain in the past which subsided on its own. Her temperature is 37°C (99.6°F), respirations are 16/min, pulse is 78/min, and blood pressure is 122/98 mm Hg. Physical examination is normal except for diffuse tenderness of her abdomen. She undergoes a limited abdominal ultrasound which reveals a 1.4 cm gallbladder polyp. What is the next best step in the management of this patient?
A 68-year-old woman comes to the emergency department because of abdominal pain for 3 days. Physical examination shows guarding and tenderness to palpation over the left lower abdomen. Test of the stool for occult blood is positive. A CT scan of the abdomen is shown. Which of the following mechanisms best explains the patient's imaging findings?

An 8-year old boy with no past medical history presents to the emergency room with 24-hours of severe abdominal pain, nausea, vomiting, and non-bloody diarrhea. His mom states that he has barely eaten in the past 24 hours and has been clutching his abdomen, first near his belly button and now near his right hip. His temperature is 101.4°F (38.5°C), blood pressure is 101/63 mmHg, pulse is 100/min, and respirations are 22/min. On physical exam, the patient is lying very still. There is abdominal tenderness and rigidity upon palpation of the right lower quadrant. What is the most likely cause of this patient’s clinical presentation?
A 44-year-old obese woman presents with abdominal pain. She says the pain started while she was having lunch at a fast-food restaurant with her children. The pain began shortly after eating and has persisted for 6 hours. She has vomited once. Her vital signs are as follows: HR 88, BP 110/70 mmHg, T 38.5°C (101.3°F). On physical exam, she is tender to palpation in the right upper quadrant of her abdomen. Her skin appears normal. Her liver function tests, amylase, and lipase levels are normal. A right upper quadrant abdominal ultrasound is challenged by her body habitus and is not able to visualize any gallstones. Which of the following is the most likely cause of her presentation?
A 55-year-old woman comes to the emergency department because of a 24-hour history of severe lower abdominal pain. She has had two episodes of nonbloody vomiting today and has been unable to keep down food or fluids. She has not had a bowel movement since the day before. She has hypertension, hyperlipidemia, and osteoarthritis. She had a cholecystectomy 5 years ago. She has smoked one pack of cigarettes daily for the last 20 years. Current medications include chlorthalidone, atorvastatin, and naproxen. Her temperature is 38.8°C (101.8°F), pulse is 102/min, respirations are 20/min, and blood pressure is 118/78 mm Hg. She is 1.68 m (5 ft 6 in) tall and weighs 94.3 kg (207.9 lbs); BMI is 33.4 kg/m2. Abdominal examination shows a soft abdomen with hypoactive bowel sounds. There is moderate left lower quadrant tenderness. A tender mass is palpable on digital rectal examination. There is no guarding or rebound tenderness. Laboratory studies show: Leukocyte count 17,000/mm3 Hemoglobin 13.3 g/dl Hematocrit 40% Platelet count 188,000/mm3 Serum Na+ 138 mEq/L K+ 4.1 mEq/L Cl- 101 mEq/L HCO3- 22 mEq/L Urea Nitrogen 18.1 mg/dl Creatinine 1.1 mg/dl Which of the following is most appropriate to confirm the diagnosis?
Practice by Chapter
Acute appendicitis
Practice Questions
Acute cholecystitis
Practice Questions
Small bowel obstruction
Practice Questions
Large bowel obstruction
Practice Questions
Mesenteric ischemia
Practice Questions
Gastrointestinal perforation
Practice Questions
Abdominal compartment syndrome
Practice Questions
Acute pancreatitis management
Practice Questions
Diverticulitis
Practice Questions
Incarcerated/strangulated hernias
Practice Questions
Non-operative management principles
Practice Questions
Diagnostic approach to acute abdomen
Practice Questions
Damage control surgery
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app