
Schizophrenia — MCQs

On this page
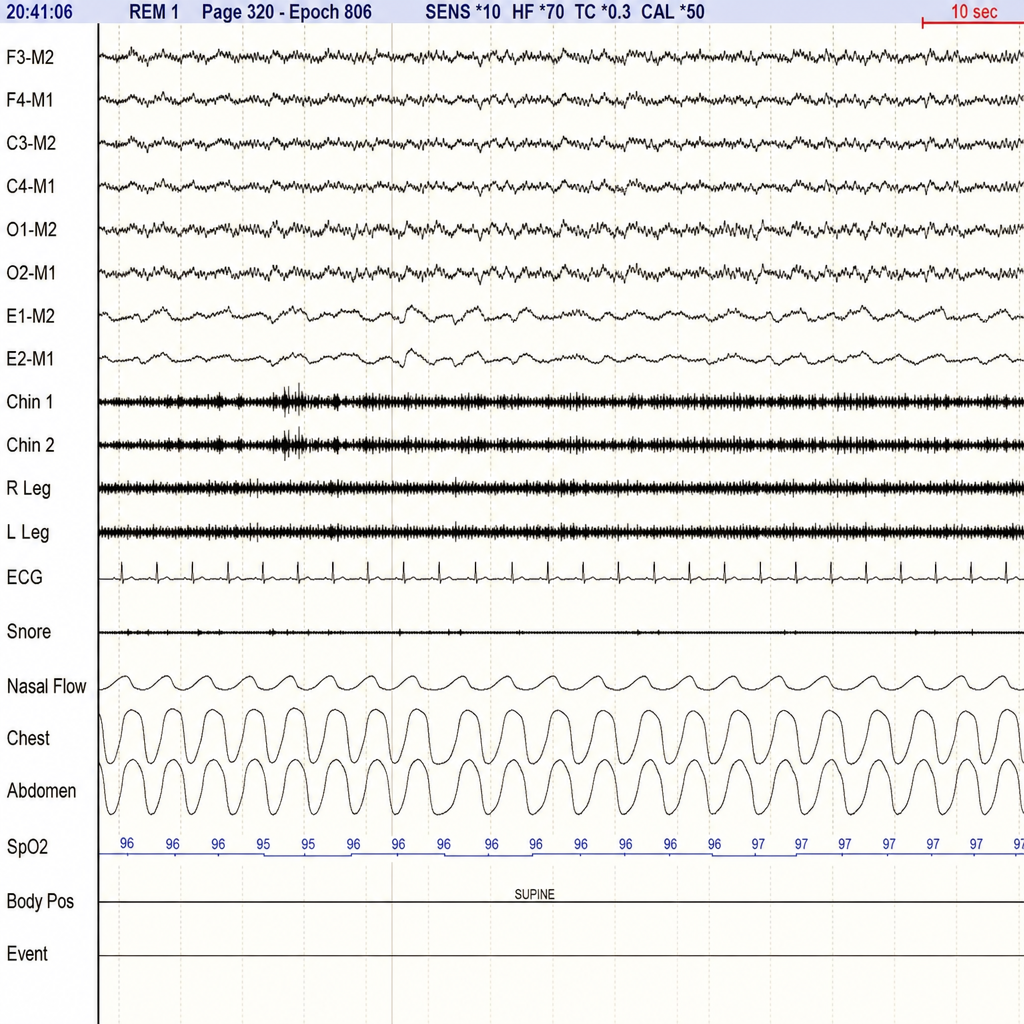
A sleep medicine clinic evaluates a 67-year-old man referred for abnormal nocturnal behaviors. His bed partner reports that he shouts, punches, and kicks during sleep, sometimes injuring himself. He does not recall the events. Polysomnography from stage R sleep demonstrates high-amplitude, mixed-frequency EEG activity with the EMG channel showing persistent tonic and phasic muscle activity in the chin and bilateral leg leads throughout the REM epoch. Apnea-hypopnea index is 3 events/hour. He takes no sedating medications. Which of the following is the most appropriate initial management?
A 24-year-old man and his mother arrive for a psychiatric evaluation. She is concerned about his health and behavior ever since he dropped out of graduate school and moved back home 8 months ago. He is always very anxious and preoccupied with thoughts of school and getting a job. He also seems to behave very oddly at times such as wearing his winter jacket in summer. He says that he hears voices but he can not understand what they are saying. When prompted he describes a plot to have him killed with poison seeping from the walls. Today, his heart rate is 90/min, respiratory rate is 17/min, blood pressure is 110/65 mm Hg, and temperature is 36.8°C (98.2°F). On physical exam, he appears gaunt and anxious. His heart has a regular rate and rhythm and his lungs are clear to auscultation bilaterally. CMP, CBC, and TSH are normal. A urine toxicology test is negative. What is the most likely diagnosis?
A 27-year-old woman comes to the physician because she has been hearing voices in her apartment during the past year. She also reports that she has been receiving warning messages in newspaper articles during this period. She thinks that “someone is trying to kill her”. She avoids meeting her family and friends because they do not believe her. She does not use illicit drugs. Physical examination shows no abnormalities. Mental status examination shows a normal affect. Which of the following is the most appropriate long-term treatment?
A 31-year-old woman comes to the physician because she thinks that her “right wrist is broken.” She says that she has severe pain and that “the bone is sticking out.” She has not had any trauma to the wrist. Her medical records indicate that she was diagnosed with schizophrenia 2 years ago and treated with olanzapine; she has not filled any prescriptions over the past 4 months. Three weeks ago, she stopped going to work because she “did not feel like getting up” in the morning. Vital signs are within normal limits. Physical examination of the right wrist shows no visible injury; there is no warmth, swelling, or erythema. Range of motion is limited by pain. On mental status examination, she has a flat affect. Her speech is pressured and she frequently changes the topic. She has short- and long-term memory deficits. Attention and concentration are poor. There is no evidence of suicidal ideation. Urine toxicology screening is negative. An x-ray of the wrist shows no abnormalities. Which of the following is the most appropriate response to this patient's concerns?
A 22-year-old man with a history of schizophrenia presents to the emergency room escorted by police. The officers state that the patient was found at a local mall, threatening to harm people in the parking lot, screaming at them, and chasing them. The patient states that those people were agents of the government sent to kill him. The patient is agitated and seems to be responding to internal stimuli. He refuses treatment and states that he wants to leave or he will hurt the hospital staff and other patients. Which of the following is the most appropriate next step in management?
A 45-year-old obese man is evaluated in a locked psychiatric facility. He was admitted to the unit after he was caught running through traffic naked while tearing out his hair. His urine toxicology screening was negative for illicit substances and after careful evaluation and additional history, provided by his parents, he was diagnosed with schizophrenia and was treated with aripiprazole. His symptoms did not improve after several dosage adjustments and he was placed on haloperidol, but this left him too lethargic and slow and he was placed on loxapine. After several dosage adjustments today, he is still quite confused. He describes giant spiders and robots that torture him in his room. He describes an incessant voice screaming at him to run away. He also strongly dislikes his current medication and would like to try something else. Which of the following is indicated in this patient?
A 31-year-old woman comes to the emergency department requesting an abortion. She hears voices telling her that she needs ""to undergo a cleanse."" She experiences daytime sleepiness because she repeatedly wakes up at night. She says that she is no longer interested in activities that she used to enjoy. About 2 months ago, her psychiatrist switched her medication from aripiprazole to risperidone because it was not effective even at maximum dose. Vital signs are within normal limits. Mental status examination shows accelerated speech, and the patient regularly switches the conversation to the natural habitat of bees. A urine pregnancy test is positive. Toxicology screening is negative. Pelvic ultrasonography shows a pregnancy at an estimated 15 weeks' gestation. Following admission to the hospital, which of the following is the most appropriate next step in management?
A 16-year-old boy is brought in to a psychiatrist's office by his mother for increasingly concerning erratic behavior. Her son has recently entered a new relationship, and he constantly voices beliefs that his girlfriend is cheating on him. He ended his last relationship after voicing the same beliefs about his last partner. During the visit, the patient reports that these beliefs are justified, since everyone at school is “out to get him.” He says that even his teachers are against him, based on their criticism of his schoolwork. His mother adds that her son has always held grudges against people and has always taken comments very personally. The patient has no psychiatric history and is in otherwise good health. What condition is this patient genetically predisposed for?
A 27-year-old woman is brought to the office at the insistence of her fiancé to be evaluated for auditory hallucinations for the past 8 months. The patient’s fiancé tells the physician that the patient often mentions that she can hear her own thoughts speaking aloud to her. The hallucinations have occurred intermittently for at least 1-month periods. Past medical history is significant for hypertension. Her medications include lisinopril and a daily multivitamin both of which she frequently neglects. She lost her security job 7 months ago after failing to report to work on time. The patient’s vital signs include: blood pressure 132/82 mm Hg; pulse 72/min; respiratory rate 18/min, and temperature 36.7°C (98.1°F). On physical examination, the patient has a flat affect and her focus fluctuates from the window to the door. She is disheveled with a foul smell. She has difficulty focusing on the discussion and does not quite understand what is happening around her. A urine toxicology screen is negative. Which of the following is the correct diagnosis for this patient?
A 24-year-old man is brought to the doctor's office by his mother because the patient believes aliens have begun to read his mind and will soon have him performing missions for them. The patient's mother says that the delusions have been intermittently present for periods of at least 1-month over the past year. When he is not having delusions, she says he still lacks expression and has no interest in socializing with his friends or going out. He has no past medical history and takes no prescription medications. The patient has smoked 1 pack of cigarettes daily for the past 10 years. Since the disturbance, he has not been able to maintain employment and lives at home with his mother. His vitals include: blood pressure 124/82 mm Hg, pulse 68/min, respiratory rate 14/min, temperature 37.3°C (99.1°F). On physical examination, the patient exhibits poor eye contact with a flat affect. His speech is circumferential, and he is currently experiencing bizarre delusions. The results from a urine drug screen are shown below: Amphetamine negative Benzodiazepine negative Cocaine negative GHB negative Ketamine negative LSD negative Marijuana negative Opioids negative PCP negative Which of the following is the correct diagnosis?
Practice by Chapter
Diagnostic criteria and subtypes
Practice Questions
Positive symptoms
Practice Questions
Negative symptoms
Practice Questions
Cognitive symptoms
Practice Questions
Prodromal phase and early intervention
Practice Questions
Neurobiological theories of schizophrenia
Practice Questions
Genetics of schizophrenia
Practice Questions
Neuroimaging findings
Practice Questions
First-generation antipsychotics
Practice Questions
Second-generation antipsychotics
Practice Questions
Treatment-resistant schizophrenia
Practice Questions
Psychosocial rehabilitation
Practice Questions
Long-acting injectable antipsychotics
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app