
Psychotic Disorders — MCQs

On this page
A 21-year-old nurse starts to feel ill during his evening shift. Earlier this evening, he started his shift in his normal state of health. Past medical history is significant for multiple admissions to the hospital under strange circumstances. One time he presented to the emergency department complaining of severe abdominal pain and gallstones, though no stones were identified and he was discharged after a full workup. Another time he was admitted for recurrent vomiting episodes and he was discharged after an EGD and several rounds of antiemetics. He has also visited an outpatient clinic for back pain and knee pain, though no findings were ever identified. He takes a multivitamin every day. His mother developed breast cancer at 47 and his father is healthy. Today, his blood pressure is 120/80 mm Hg, heart rate is 105/min, respiratory rate is 17/min, and temperature is 36.9°C (98.4°F). On physical exam, he appears thin and anxious. He is diaphoretic with clammy hands. His heart is tachycardic with an irregular rhythm and his lungs are clear to auscultation bilaterally. A urine toxicology test and EKG are negative. Random blood sugar is 45 mg/dL. The nurse is admitted and treated appropriately. After a thorough review of his medical records, the hospitalist assigned to this patient consults with psychiatry because she is concerned the patient may have factitious disorder. Which of the following would confirm a diagnosis of the factitious disorder in this patient?
A 21-year-old woman is brought to the clinic for evaluation by her brother. The patient’s brother says that, 3 days ago, the patient had put on her best pantsuit and makeup and insisted that she was returning to work and driving to Seattle to take over for the CEO of the Amazon Corporation. He says this was especially odd because her husband was just killed in an automobile accident in a different city 2 days ago. Today, the patient’s brother says she was saddened, wearing grey jogging pants. The patient says she does not recall acting odd and does remember that her husband is dead. Her vital signs include: blood pressure 132/84 mm Hg, pulse 92/min, respiratory rate 16/min, temperature 37.4°C (99.4°F). Upon physical examination, the patient’s affect is saddened but her speech rate and volume are normal. There is no hallucinations, mania, interruptive speech, depressive symptoms, or loss of interest in activities once enjoyed. Results of urine drug screen are provided below: Amphetamine negative Benzodiazepine negative Cocaine negative GHB negative Ketamine negative LSD negative Marijuana negative Opioids negative PCP negative Which of the following best describes the patient’s state?
A mother brings her 4-year-old son to his pediatrician. Over the last eight months, her son has been exhibiting several "odd" behaviors. Most importantly, he repeatedly says that he is playing games with a friend named "Steven," though she is certain that he does not exist. She has often found him acting out magical scenarios as though someone else is present, when no one is there. What is the most likely diagnosis in this patient?
A 45-year-old man presents to a psychiatrist by his wife with recent behavioral and emotional changes. The patient’s wife says that her husband’s personality has completely changed over the last year. She also says that he often complains of unpleasant odors when actually there is no discernible odor present. The patient mentions that he is depressed at times while on other occasions, he feels like he is ‘the most powerful man in the world.’ The psychiatrist takes a detailed history from this patient and concludes that he is most likely suffering from a psychotic disorder. However, before prescribing an antipsychotic medication, he recommends that the patient undergoes brain imaging to rule out a brain neoplasm. Based on the presence of which of the following clinical signs or symptoms in this patient is the psychiatrist most likely recommending this imaging test?
A 23-year-old man is brought to the emergency department by his girlfriend because of acute agitation and bizarre behavior. The girlfriend reports that, over the past 3 months, the patient has become withdrawn and stopped pursuing hobbies that he used to enjoy. One month ago, he lost his job because he stopped going to work. During this time, he has barely left his apartment because he believes that the FBI is spying on him and controlling his mind. He used to smoke marijuana occasionally in high school but quit 5 years ago. Physical and neurologic examinations show no abnormalities. On mental status examination, he is confused and suspicious with marked psychomotor agitation. His speech is disorganized and his affect is labile. Which of the following is the most likely diagnosis?
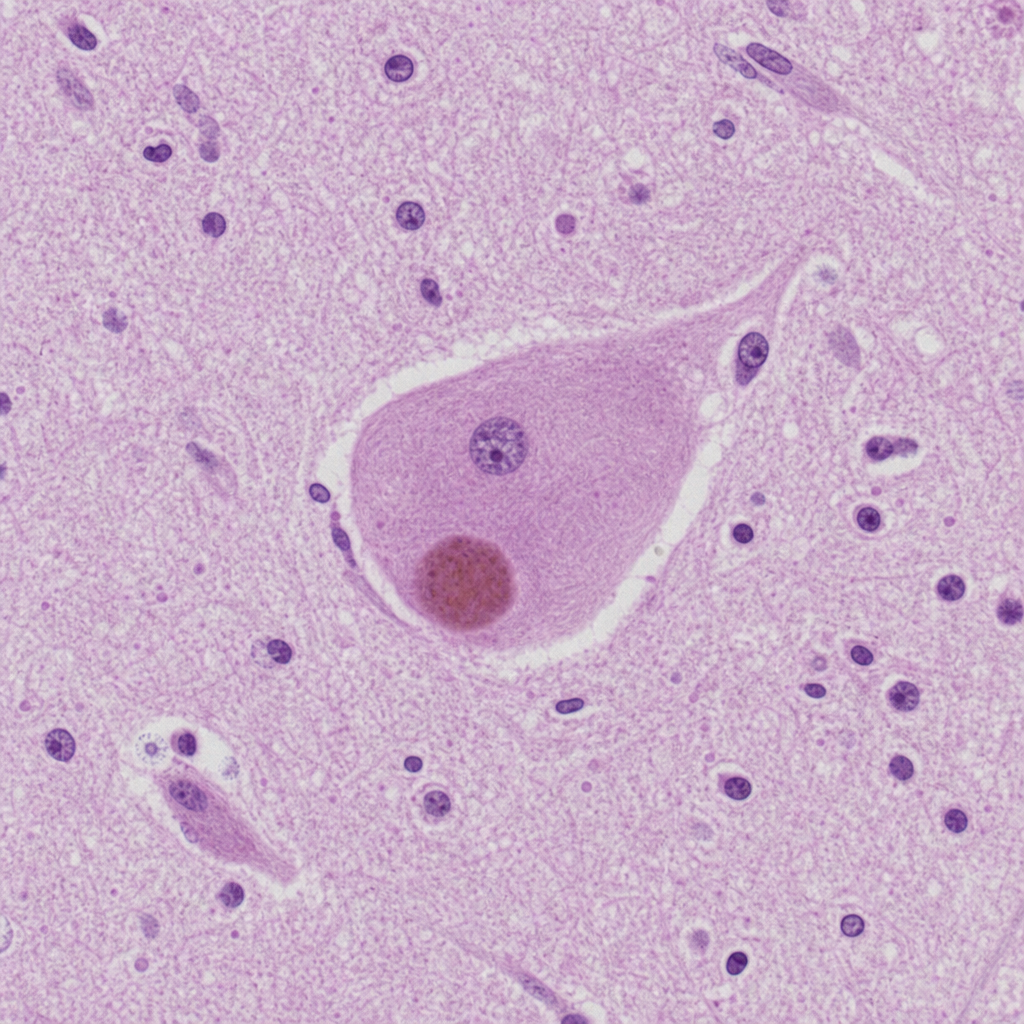
An 81-year-old man is brought to the physician by his daughter after he was found wandering on the street. For the last 3 months, he often has a blank stare for several minutes. He also claims to have seen strangers in the house on several occasions who were not present. He has hypertension and hyperlipidemia, and was diagnosed with Parkinson disease 8 months ago, with parkinsonian motor symptoms beginning approximately 10 months ago. His current medications include carbidopa-levodopa, hydrochlorothiazide, and atorvastatin. His blood pressure is 150/85 mm Hg. He has short-term memory deficits and appears confused and disheveled. Examination shows bilateral muscle rigidity and resting tremor in his upper extremities. He has a slow gait with short steps. Microscopic examination of the cortex of a patient with the same condition is shown. Which of the following is the most likely diagnosis?
A 21-year-old man is brought to the office by his parents due to concerns about his behavior. They describe their son as aloof and a loner who earns average to below average grades in school. Today, his heart rate is 90/min, respiratory rate is 17/min, blood pressure is 110/65 mm Hg, and temperature is 36.8°C (98.2°F). On physical examination, he appears gaunt and anxious. His heart has a regular rhythm, and his lungs are clear to auscultation bilaterally. CMP, CBC, and TSH are normal. A urine toxicology test is negative. During the examination, he avoids eye contact and appears detached. When asked about his social life, he claims that he does not care about making friends and prefers to be alone. He says he enjoys going to the movies, but he enjoys doing this alone. He has not had a romantic partner before and takes little pleasure in intimacy. He denies experiencing hallucinations or delusions. Which of the following is the most likely diagnosis?
A 27-year-old female is brought to the Emergency Department by Fire Rescue after participating in a physical altercation with several commuters on the subway. She appears to be responding to hallucinations and is diaphoretic. Her vitals are as follows: T 100.5F (38C), HR 115, BP 155/90, RR 17. Her past medical history is notable for a previous ED visit for phencyclidine-related agitation. Which of the following physical findings would most strongly suggest the same diagnosis?
A 35-year-old male with a history of repeated arrests for assault, robbery, and arson displays a callous disregard for the safety of others and a lack of remorse, as evidenced by smiling when questioned about burning down his ex-girlfriend's apartment. Considering a diagnosis of antisocial personality disorder, which of the following behaviors was most likely present during his childhood?
A 26-year-old woman is brought to the emergency department by her husband due to her disturbing behavior over the past 24 hours. Her husband says that he has noticed his wife talking to herself and staying in a corner of a room throughout the day without eating or drinking anything. She gave birth to their son 2 weeks ago but has not seen or even acknowledged her baby’s presence ever since he was born. He says that he didn’t think much of it because she seemed overwhelmed during her pregnancy and he considered that she was probably unable to cope with being a new mother; however, last night, he says, his wife told him that their child was the son of the devil and they ought to get rid of him as soon as possible. Which of the following describes this patient’s abnormal reaction to her child?
Practice by Chapter
Brief psychotic disorder
Practice Questions
Schizophreniform disorder
Practice Questions
Schizoaffective disorder
Practice Questions
Substance-induced psychotic disorder
Practice Questions
Psychosis due to medical conditions
Practice Questions
Catatonia across disorders
Practice Questions
First-episode psychosis management
Practice Questions
Metabolic monitoring in psychotic disorders
Practice Questions
Antipsychotic mechanisms of action
Practice Questions
Antipsychotic side effect management
Practice Questions
Violence risk assessment in psychosis
Practice Questions
Cognitive remediation in psychotic disorders
Practice Questions
Family interventions for psychotic disorders
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app