
Neurodevelopmental disorders (ADHD, autism) — MCQs

On this page
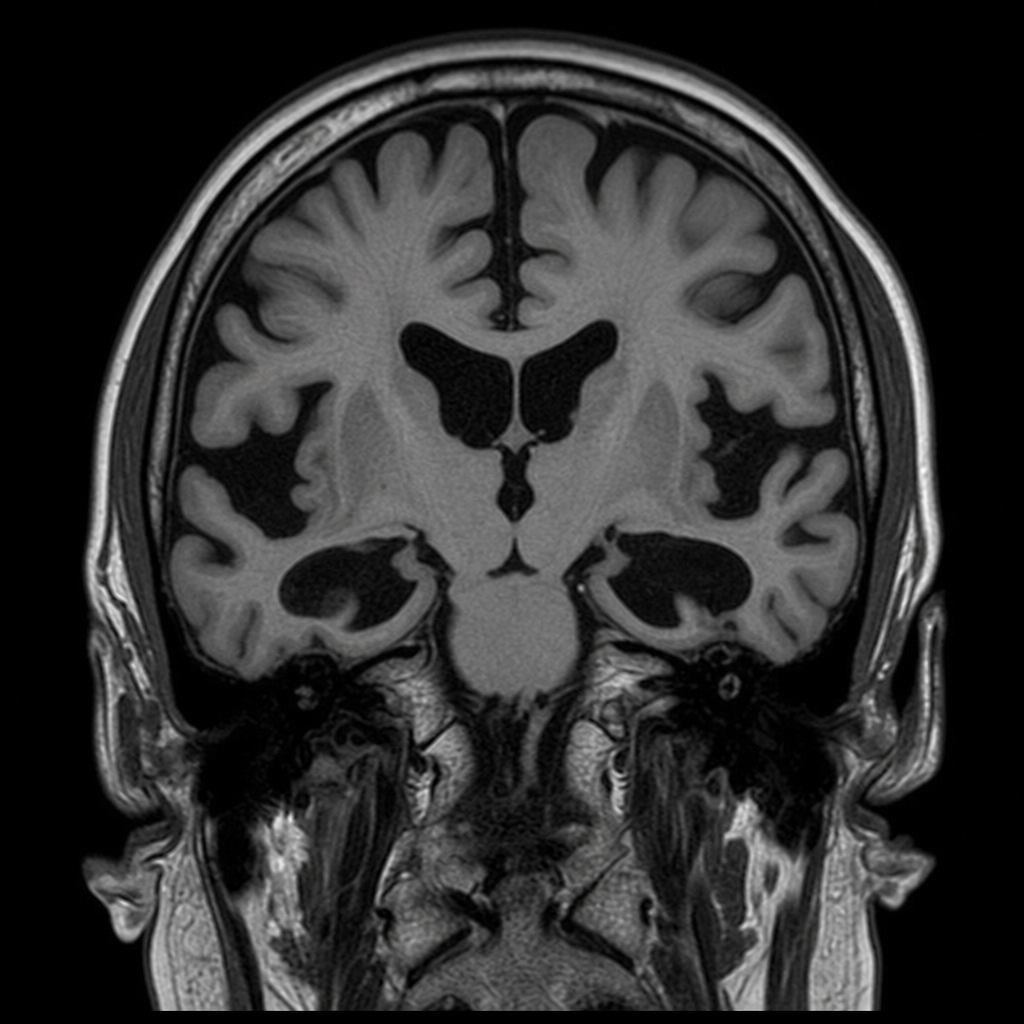
A 67-year-old retired engineer is brought by his daughter for a 14-month history of progressive personality change. She reports he has become disinhibited, made sexually inappropriate comments at family gatherings, and recently shoplifted a candy bar without apparent concern. He scores 24/30 on the MoCA, losing points primarily in the executive function and abstraction domains. Memory is relatively preserved. He has no history of stroke, head trauma, or alcohol use. An MRI of the brain shows frontal and anterior temporal lobe atrophy with relative sparing of the posterior cortex and hippocampi. Which of the following is the most likely underlying diagnosis?
A 4-year-old boy presents with language delay, toe-walking, hand-flapping, and intense interest in trains. He makes poor eye contact but occasionally engages in joint attention with his mother when looking at trains. He has sensory sensitivities to loud noises. He can identify all letters and numbers but cannot have reciprocal conversations. His Childhood Autism Rating Scale (CARS) score is borderline. His parents request your opinion on diagnosis and intervention priorities given diagnostic uncertainty and limited early intervention resources in their area.
A 15-year-old girl with ADHD-predominantly inattentive type has tried methylphenidate, amphetamine salts, and atomoxetine with partial response or intolerable side effects. She has comorbid anxiety disorder and mild depression. She is motivated for treatment and has good family support. Her psychiatrist considers guanfacine as next-line therapy. Evaluate the appropriateness of this choice given her clinical profile.
A 12-year-old boy with autism spectrum disorder and intellectual disability is hospitalized for severe aggression. He is nonverbal and communicates through an augmentative device. Behavioral interventions have failed. He has been on risperidone 3 mg daily for 2 months with minimal improvement. His team considers adding a second medication. He has gained 8 kg, developed elevated prolactin (78 ng/mL), and shows early signs of gynecomastia. What is the most appropriate management strategy?
A 9-year-old boy with ADHD treated with methylphenidate develops vocal tics (throat clearing) and motor tics (eye blinking) after 8 months of treatment. His ADHD symptoms are well-controlled, but the tics are becoming socially problematic. His father had transient tics as a child. Neurological examination shows the tics but is otherwise normal. What factor most strongly suggests the tics are unmasked Tourette disorder rather than medication-induced?
A 5-year-old boy with autism spectrum disorder has severe self-injurious behavior including head-banging that has resulted in two emergency department visits. Intensive behavioral therapy has been partially effective. His parents are concerned about medication side effects but are desperate for improvement. Analysis of behavior logs shows the self-injury increases when demands are placed on him and decreases with sensory activities. What medication choice and rationale is most appropriate?
A 10-year-old girl is evaluated for academic difficulties. Her teacher reports she often daydreams, misses instructions, and makes careless errors despite adequate intelligence. She is well-behaved, quiet, and never disruptive. At home, she forgets daily tasks, frequently loses items, and has difficulty organizing schoolwork. Her mother had similar problems as a child. On examination, she is cooperative but appears distracted. What feature of her presentation would most strongly differentiate her ADHD subtype from the combined presentation?
A 6-year-old boy with autism spectrum disorder is brought for evaluation of new-onset aggression toward peers at school. He has limited verbal communication and becomes aggressive when transitions occur without warning. His special education teacher notes the aggression typically occurs during unstructured activities. Applied behavioral analysis has been partially helpful. What is the most appropriate next step in management?
An 8-year-old boy with ADHD has been taking methylphenidate for 6 months with good symptom control at school. His parents report he has lost 4 kg and his growth chart shows he has dropped from the 60th to the 25th percentile for weight. His appetite is significantly decreased, particularly at lunch. What is the most appropriate management approach?
A 4-year-old girl is evaluated for delayed speech development. She has a 10-word vocabulary and does not combine words. She avoids eye contact, engages in repetitive hand-flapping, and becomes distressed when her daily routine changes. She lines up her toys repeatedly rather than engaging in pretend play. She does not respond to her name but is not deaf. Her motor milestones were normal. What is the most likely diagnosis?
Practice by Chapter
ADHD subtypes and diagnostic criteria
Practice Questions
Neurobiology of ADHD
Practice Questions
Stimulant medications
Practice Questions
Non-stimulant ADHD treatments
Practice Questions
Autism spectrum disorder diagnostic criteria
Practice Questions
Autism assessment tools
Practice Questions
Early intervention in ASD
Practice Questions
Applied behavior analysis
Practice Questions
Intellectual disability classification
Practice Questions
Learning disorders
Practice Questions
Communication disorders
Practice Questions
Motor disorders (tic disorders, stereotypic movement)
Practice Questions
Transition to adult care
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app