
Mood Disorders — MCQs

On this page
A 15-year-old boy is brought to the physician by his mother because of 4 months of strange behavior. She says that during this period, he has had episodic mood swings. She has sometimes found him in his room “seemingly drunk” and with slurred speech. These episodes usually last for approximately 15 minutes, after which he becomes irritable. He has had decreased appetite, and his eyes occasionally appear red. He has trouble keeping up with his schoolwork, and his grades have worsened. Physical examination shows an eczematous rash between the upper lip and nostrils. Neurologic examination shows a delay in performing alternating palm movements. Use of which of the following is the most likely cause of this patient's condition?
A 68-year-old man seeks evaluation by a physician with complaints of worsening forgetfulness and confusion for 1 year. According to his wife, he has always been in good health and is generally very happy; however, he has started to forget important things. He recently had his driving license revoked because of multiple tickets, but he cannot recall having done anything wrong. This morning, he neglected to put on his socks and was quite agitated when she pointed this out to him. He denies having a depressed mood, sleep problems, or loss of interest. He occasionally has a glass of wine with dinner and has never smoked or used recreational drugs. His medical history and family medical history are unremarkable. His pulse is 68/min, respirations are 14/min, and blood pressure is 130/84 mm Hg. Except for a mini-mental state examination (MMSE) score of 20/30, the remainder of the physical examination is unremarkable. Imaging studies, including a chest X-ray and CT of the brain, reveal no pathologic findings. An electrocardiogram (ECG) is also normal. Laboratory testing showed the following: Serum glucose (fasting) 76 mg/dL Serum electrolytes: Sodium 140 mEq/L Potassium 4.1 mEq/L Chloride 100 mEq/L Serum creatinine 0.9 mg/dL Blood urea nitrogen 11 mg/dL Cholesterol, total: 180 mg/dL HDL-cholesterol 45 mg/dL LDL-cholesterol 75 mg/dL Triglycerides 135 mg/dL Hemoglobin (Hb%) 16 g/dL Mean corpuscular volume (MCV) 85 fL Reticulocyte count 0.9% Erythrocyte count 5 million/mm³ Thyroid-stimulating hormone 3.5 µU/mL Urinalysis Glucose Negative Ketones Negative Leucocytes Negative Nitrite Negative RBCs Negative Casts Negative Which of the following is the most likely diagnosis?
An 8-year-old boy is brought to the clinic by his father for an annual well-check. His dad reports that he has been "difficult to handle" as he would not listen and follow instructions at home. "Telling him to sit still and do something is just so hard," the father says. His teacher also reports difficulties in the classroom where the child would talk out of turn and interrupt the class intermittently by doing something else. His grades have been suffering as a result. Otherwise, the patient has been healthy and up to date on his immunizations. What is the best course of management for this patient?
An 11-year-old boy is brought to the doctor by his father because his father is worried about the boy's performance in school and his lack of a social life. His father is also worried about the ongoing bullying his son is experiencing due to swearing outbursts the boy has exhibited for several years. During these outbursts, the boy contorts his face, blinks repeatedly, and grunts. His father is worried that the bullying will worsen and would like to see if there is a medication that can help his son. Which of the following medications is most likely to be beneficial?
A 50-year-old female radiologist who is interviewing for a night shift position states that she was fired from her past 3 previous positions because she had difficulty working with others. She states that she is perfect for this job however, as she likes to work on her own and be left alone. She emphasizes that she does not have any distractions or meaningful relationships, and therefore she is always punctual and never calls in sick. She is not an emotional individual. Which of the following personality disorders best fits this female?
A 53-year-old man is brought to the clinic by his son for the evaluation of unusual behavior. He is a shopkeeper by profession and sometimes behaves very rudely to the customers. Recently, he accused one of the customers of using black magic over his shop. He has been increasingly irritable, forgetting things, and having problems managing his finances over the past 8 months. He is also having difficulty finding words and recalling the names of objects during the conversation. There is no history of recent head trauma, fever, hallucinations, or abnormal limb movements. Past medical history is significant for a well-controlled type 2 diabetes mellitus. Family history is unremarkable. He does not smoke or use illicit drugs. Vital signs are stable with a blood pressure of 134/76 mm Hg, a heart rate of 88/min, and a temperature of 37.0°C (98.6°F). On physical examination, he has problems naming objects and planning tasks. Mini-mental state examination (MMSE) score is 26/30. Cranial nerve examination is normal. Muscle strength is normal in all 4 limbs with normal muscle tone and deep tendon reflexes. Sensory examination is also normal. What is the most likely diagnosis?
A 37-year-old woman is brought to the physician for worsening depressive mood and irritability. Her mood changes began several months ago. Her husband has also noticed shaky movements of her limbs and trunk for the past year. The patient has no suicidal ideation. She has no history of serious illness and takes no medications. Her father died by suicide at the age of 45 years. Her temperature is 37°C (98.6°F), pulse is 76/min, and blood pressure is 128/72 mm Hg. She speaks slowly and quietly and only looks at the floor. She registers 3/3 words but can recall only one word 5 minutes later. Examination shows irregular movements of the arms and legs at rest. Extraocular eye movements are normal. Muscle strength is 5/5 throughout, and deep tendon reflexes are 2+ bilaterally. Further evaluation is most likely to show which of the following?
A 66-year-old man comes to the physician for a follow-up examination after a below-knee amputation of the right lower leg. Three weeks ago, he had an acute arterial embolism that could not be revascularized in time to save the leg. He now reports episodic hot, shooting, and tingling pain in the right lower leg that began shortly after the amputation. He has type 2 diabetes mellitus. He has smoked one pack of cigarettes daily for the past 30 years. His current medications are metformin and prophylactic subcutaneous heparin. His temperature is 37.1°C (98.8°F), pulse is 78/min, and blood pressure is 135/88 mm Hg. Physical examination shows a slightly erythematous stump with clean sutures. The skin overlying the stump is warm and well-perfused. Muscle strength and sensation are normal throughout the remaining extremity and the left lower extremity. Which of the following is the most likely diagnosis?
An 8-year-old boy is brought to the physician by his foster mother because of complaints from his teachers regarding poor performance at school for the past 8 months. He does not listen to their instructions, often talks during class, and rarely completes his school assignments. He does not sit in his seat in the classroom and often cuts in line at the cafeteria. His foster mother reports that he runs around a lot inside the house and refuses to help his sister with chores and errands. He frequently interrupts his foster mother's conversations with others and talks excessively. She has found him trying to climb on the roof on multiple occasions. He was placed in foster care because of neglect by his biological parents 3 years ago. Physical examination shows no abnormalities. Neurologic examination shows no focal findings. Mental status examination shows a neutral affect. Which of the following is the most likely diagnosis?
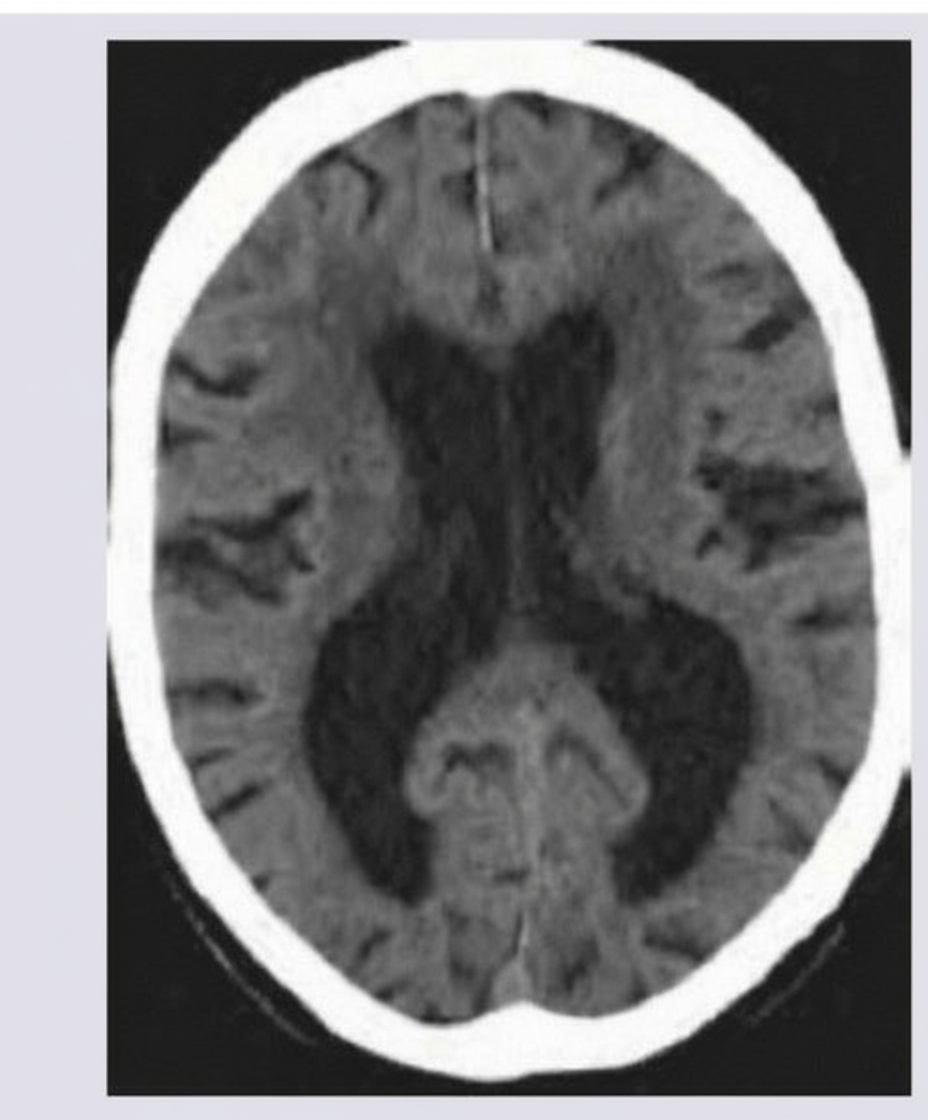
An 88-year-old man is brought to his primary care physician by his son. The patient has been in excellent health his entire life, but in the last few years appears to have grown steadily confused. He frequently calls his son about things that they have already discussed, forgets where he has placed his keys, and recently the patient's son noticed several unpaid bills on the patient's desk at home. The patient is upset at being "dragged" into see the physician and claims that everything is fine--he is just "getting older". A complete neurologic exam is normal except for significant difficulty with recall tasks. In the course of the medical work-up, you obtain a CT scan and see the findings in figure A. What is the most likely cause of this patient's CT findings?
Practice by Chapter
Persistent depressive disorder (dysthymia)
Practice Questions
Premenstrual dysphoric disorder
Practice Questions
Disruptive mood dysregulation disorder
Practice Questions
Adjustment disorder with depressed mood
Practice Questions
Substance-induced mood disorders
Practice Questions
Mood disorders due to medical conditions
Practice Questions
Bereavement and complicated grief
Practice Questions
Mood disorder epidemiology
Practice Questions
Cultural aspects of mood disorders
Practice Questions
Child and adolescent mood disorders
Practice Questions
Geriatric mood disorders
Practice Questions
Comorbidities with mood disorders
Practice Questions
Functional impairment assessment
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app