
Mood Disorders — MCQs

On this page
A 38-year-old male presents for counseling by a psychologist mandated by the court. The patient explains that he does not mean to hit his wife when they are arguing, but something just comes over him that he cannot control. Upon further discussion, the patient reveals that his father was incarcerated several times for physically abusing his mother. Which of the following best describes the behavior seen in this patient?
You are a sleep physician comparing the results of several hypnograms taken in the sleep lab the prior night. You examine one chart which shows decreased REM sleep, less total time sleeping, and more frequent nocturnal awakenings. Which of these patients most likely exhibits this pattern?
A 18-year-old woman presents to her primary care physician reporting that she has not experienced her first menses. She is accompanied by her mother who states that she personally experienced menstruation at age 12 and that the patient's sister started menstruating at the age of 11 years. The patient is not sexually-active and denies taking any medications. On physical examination, the patient appears thin and has fine hair covering her arms. Her height is 62 inches (157.48 cm) and her weight is 85 pounds (38.5 kg). The patient does not make eye contact and only answers in one word responses. The mother is asked to step out of the room and the interview resumes. After establishing some trust, the patient admits that she does not have an appetite. She has had difficulty sleeping and some feels guilty for worrying her mother. She also admits to occasional cocaine use. She switches between binge-eating and vomiting. She is constantly fatigued but she also goes to the gym three times daily, often without her parents’ knowledge. Which of the following is the most likely diagnosis in this patient?
A 27-year-old woman presents to your office complaining of right arm numbness and weakness. Her past medical history is unremarkable. Her family history, however, is significant for the unexpected death of both her parents at age 59 in a motor vehicle accident last week. On physical exam, her bicep, brachioradialis, and patellar reflexes are 2+ bilaterally. CNS imaging shows no abnormalities. Which of the following is the most likely diagnosis?
An 8-year-old girl presents to the psychiatrist to discuss the recent divorce of her parents. The girl explains that her mother is the most caring and loving mother anyone could ever have and that she will be spending the majority of her time with her mother. On the other hand, she exclaims that her father is an evil person and hates him. Which of the following ego defenses is best demonstrated by this girl?
A 13-year-old boy is brought to the physician by his parents for the evaluation of multiple behavioral problems. The parents report that their son has been bullying several classmates at school over the past year. During this period, he has been accused twice of stealing items from a local store. He has also beaten up the neighbor's son for no obvious reason. The parents state that they had to give up their dog for adoption after finding out that their son was torturing him. There is no personal or family history of serious illness. He attends a local middle school and his performance at school is poor compared to his classmates. He often forgets to do his homework and argues with his teachers. He was also caught smoking cigarettes. Vital signs are within normal limits. Physical examination shows no abnormalities. He has poor attention and does not answer some of the questions. For questions he answers affirmatively about his actions, he sometimes replies, “So what?.” Which of the following conditions is this patient most likely to develop?
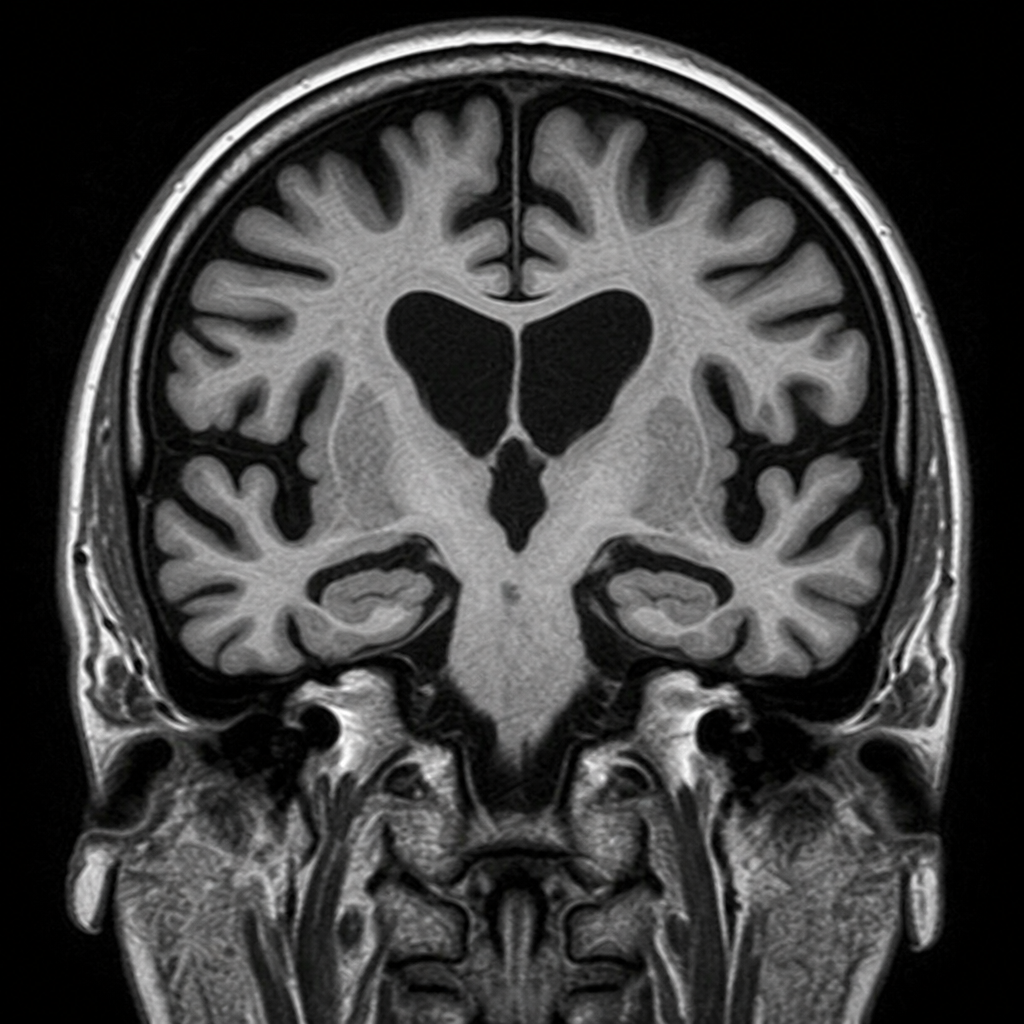
A 73-year-old man is brought to the physician by his daughter for evaluation of increasing forgetfulness during the past 6 months. The daughter reports that he recently got lost while walking home from the grocery store. He has also been more irritable recently. On mental status examination, he has a normal affect. He is oriented to person and place but cannot recall which month it is. He recalls memories from more than 20 years ago in great detail but cannot state his home address or the name of his recently born grandson. His gait is normal and there is no nystagmus. An MRI of the brain is shown. Which of the following is the most likely underlying cause of the radiologic findings?
A 24-year-old woman visits her psychiatrist a week after she delivered a baby. She is holding her baby and crying as she waits for her appointment. She tells her physician that a day or so after her delivery, she has been finding it difficult to contain her feelings. She is often sad and unable to contain her tears. She is embarrassed and often starts crying without any reason in front of people. She is also anxious that she will not be a good mother and will make mistakes. She hasn’t slept much since the delivery and is often stressed about her baby getting hurt. She makes excessive attempts to keep the baby safe and avoid any mishaps. She does not report any loss of interest in her activities and denies any suicidal tendencies. Which of the following is best course of management for this patient?
A 13-year-old boy is brought to the physician by his mother because she is concerned about her son's behavior. She reports that he has been wearing her dresses at home and asks to be called Lilly. He also stopped going to swim class because he “doesn't feel comfortable in swim trunks.” Since starting puberty about a year ago, he has not had any friends and the teachers report he is consistently being bullied at school. His academic performance has been poor for the last year even though he had maintained an A average the year before. The mother further reports that her son has had mainly female friends since preschool. She also mentions that as a child her son never enjoyed playing with typical boy toys like cars and instead preferred dressing up dolls. The patient was raised by his single mother from the age of 8 because his father left the family due to financial issues. He appears shy. Physical examination shows normal male external genitalia. There is scarce coarse, dark axillary and pubic hair. Upon questioning, the patient reports that he would rather be a girl. Which of the following is the most likely diagnosis?
A 15-year-old boy is referred to a child psychologist because of worsening behavior and constant disruption in class. He has received multiple reprimands in the past 6 months for not doing the homework his teacher assigned, and he refuses to listen to the classroom instructions. Additionally, his teachers say he is very argumentative and blames other children for not letting him do his work. He was previously well behaved and one of the top students in his class. He denies any recent major life events or changes at home. His past medical history is noncontributory. His vital signs are all within normal limits. Which of the following is the most likely diagnosis?
Practice by Chapter
Persistent depressive disorder (dysthymia)
Practice Questions
Premenstrual dysphoric disorder
Practice Questions
Disruptive mood dysregulation disorder
Practice Questions
Adjustment disorder with depressed mood
Practice Questions
Substance-induced mood disorders
Practice Questions
Mood disorders due to medical conditions
Practice Questions
Bereavement and complicated grief
Practice Questions
Mood disorder epidemiology
Practice Questions
Cultural aspects of mood disorders
Practice Questions
Child and adolescent mood disorders
Practice Questions
Geriatric mood disorders
Practice Questions
Comorbidities with mood disorders
Practice Questions
Functional impairment assessment
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app