
Mood Disorders — MCQs

On this page
A 15-year-old girl is brought into her pediatrician's office by her mother because the mother thinks her daughter has attention issues. The mother explains that her daughter started high school four months ago and had lackluster grades in a recent progress report despite having earned consistent top marks in middle school. The mother complains that her daughter never talks to her at home anymore. The patient yells at her mother in the exam room, and the mother is escorted out of the room. The patient scoffs that her mother is so overbearing, ruining her good days with criticism. She begins to chew gum and states that she hates hanging out with the girls on the cheerleading squad. She denies experiencing physical abuse from anyone or having a sexual partner. She has seen kids smoke marijuana underneath the football field bleachers, but does not go near them and denies smoking cigarettes. She denies any intention to harm herself or others, thinks her grades went down because her teachers are not as good as her middle school teachers, and states she thinks she learns best by watching explanations through online videos. What is the most likely diagnosis?
A 55-year-old man is brought to the physician because of inappropriate behavior for the past 6 months. He has been making inappropriate comments and jokes while talking to friends and family members. He was arrested 3 weeks ago while trying to kiss strangers on the street. He has no interest in talking to his daughter or playing with his grandchildren. During this period, he has developed a strong desire for chocolate pudding and potato chips and has gained 10 kg (22 lb). He appears unkempt. Vital signs are within normal limits. Physical examination is unremarkable. Mental status examination shows apathy and a blunt affect. He avoids answering questions and instead comments on the individuals he saw in the waiting room. Mini-Mental State Examination score is 28/30. A complete blood count and serum concentrations of glucose, creatinine, and electrolytes are within the reference range. Which of the following is the most likely diagnosis?
A 15-year-old girl presents to her primary care physician, accompanied by her mother, for 4 days of abdominal pain. She describes the pain as diffuse, dull, and constant. She also endorses constipation over this time. The patient's mother says the patient has become increasingly self-conscious of her appearance since starting high school this year and has increasingly isolated herself to her room, rarely spending time with or eating meals with the rest of the family. Her temperature is 98.0°F (36.7°C), blood pressure is 100/70 mmHg, pulse is 55/min, and respirations are 19/min. Body mass index (BMI) is at the 4th percentile for age and gender. Physical exam reveals dental caries, mild abdominal distension, and diffuse, fine body hair. Basic labs are most likely to reveal which of the following?
A 53-year-old man is brought to the physician by his wife because of strange behavior and emotional outbursts for the past 6 months. He was previously healthy and physically active, but he recently started binge-eating candy and stopped exercising. He was fired from his job for inappropriate behavior after he undressed in the office and made lewd remarks to several female coworkers. He claims there is nothing wrong with his behavior. On mental status examination, he is alert and irritable but cooperative. Short-term recall is normal but he has some word-finding difficulties. Babinski reflex is positive bilaterally. This patient's symptoms are most likely due to a degenerative process in which of the following regions of the brain?
A parent-teacher conference is called to discuss the behavior of a 9 year-old boy. According to the boy's teacher, he has become progressively more disruptive during class. When asked to help clean up or read out-loud, he replies with "You're not the boss of me." or "You can't make me." He refuses to participate in gym class, but will play the same games during recess. He gets along with and is well-liked by his peers. His mother reports that her son can "sometimes be difficult," but he is helpful around the house and is very good playing with his 7-year-old sister. What is the most likely diagnosis?
A 25-year-old man presents to his primary care physician for trouble with focus and concentration. The patient states that he has lived at home with his parents his entire life but recently was able to get a job at a local factory. Ever since the patient has started working, he has had trouble focusing at his job. He is unable to stay focused on any task. His boss often observes him "daydreaming" with a blank stare off into space. His boss will have to yell at him to startle him back to work. The patient states that he feels fatigued all the time and sometimes will suddenly fall asleep while operating equipment. He has tried going to bed early for the past month but is unable to fall asleep until two hours prior to his alarm. The patient fears that if this continues he will lose his job. Which of the following is the best initial step in management?
A 9-year-old boy is brought to a psychologist by his mother because his teachers frequently complain about his behavioral problems at school. The patient’s mother reports that his concerning behavior started at a young age. She says he is disrespectful to family members and to his teachers at school. He also talks back to everyone. Grounding him and limiting his freedom has not improved his behavior. His grades have never been very good, and he is quite isolated at school. After a further review of the patient’s medical history and a thorough physical exam, the physician confirms the diagnosis of oppositional defiant disorder. Which of the following additional symptoms would most likely present in this patient?
A 13-year-old teenage girl was brought to the emergency department by her mom after she collapsed. Her mom reports that she was at a birthday party when all of a sudden she fell. She reported left foot weakness and has been limping ever since. The patient has been healthy and had an uncomplicated birth history, though her mom reports that she just recovered from a cold. She currently lives with her younger sister and mother as her parents recently divorced. She does well in school and has a handful of good friends. Her physical exam demonstrated normal bulk and tone, 5/5 strength in all motions, 2+ and symmetric reflexes at biceps, triceps and knees. She had 1+ ankle reflex on left. What is the most likely explanation for her symptoms?
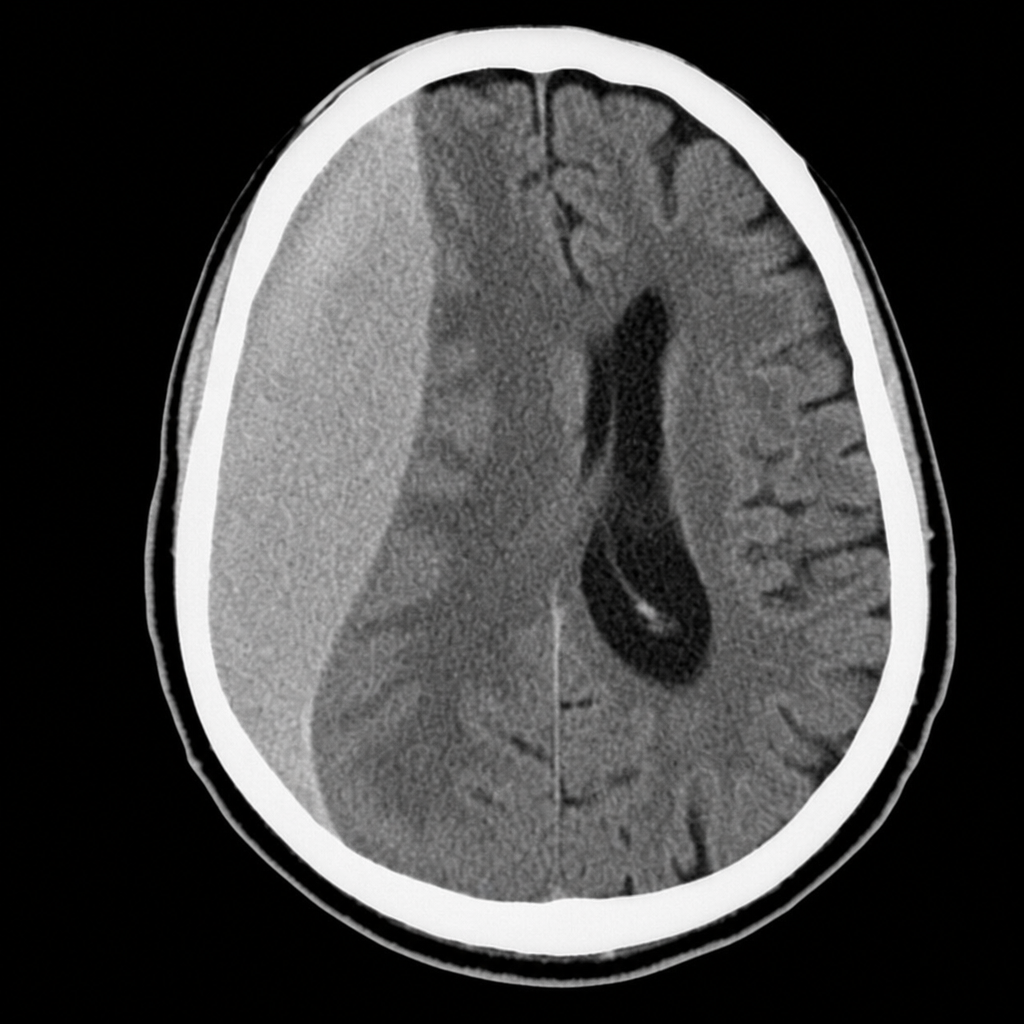
A 68-year-old man is brought to the clinic by his daughter who has noticed behavioral changes and frequent headaches for the past 2 weeks. The patient's daughter says he has been having memory and simple calculation issues, gets upset easily, and his grip strength has dramatically declined. The patient was completely normal prior to these recent changes and used to be able to perform his activities of daily living without a problem. He has a past medical history significant for hypertension, stable angina, and benign prostatic hypertrophy, as well as frequent falls with the last one occurring 1 month ago. Physical examination is remarkable for dyscalculia, short-term memory deficits, and decreased grip strength (4/5) in his right hand. A noncontrast CT of the head is performed and is shown in the image. Which of the following is the most likely etiology of this patient condition?
A 28-year-old woman is brought into the clinic by her husband with concerns that she might be depressed. She delivered a healthy newborn a week and a half ago without any complications. Since then, she has been having trouble sleeping, eating poorly, and has stopped playing with the baby. The patient says she feels like she is drained all the time and feels guilty for not doing more for the baby. Which of the following is the best course of treatment for this patient?
Practice by Chapter
Persistent depressive disorder (dysthymia)
Practice Questions
Premenstrual dysphoric disorder
Practice Questions
Disruptive mood dysregulation disorder
Practice Questions
Adjustment disorder with depressed mood
Practice Questions
Substance-induced mood disorders
Practice Questions
Mood disorders due to medical conditions
Practice Questions
Bereavement and complicated grief
Practice Questions
Mood disorder epidemiology
Practice Questions
Cultural aspects of mood disorders
Practice Questions
Child and adolescent mood disorders
Practice Questions
Geriatric mood disorders
Practice Questions
Comorbidities with mood disorders
Practice Questions
Functional impairment assessment
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app