
Newborn Screening — MCQs

The following cost-effective investigations are routinely recommended in the screening of antenatal mothers, EXCEPT:
Which diagnostic tool is preferred for metabolic disease screening in children?
An infant presented with vomiting, malnutrition, blue eyes, blonde hair & fair skin. On investigation, Guthrie test was positive. All are true regarding this disease EXCEPT:
Screening for colorectal cancer is recommended when?
Which of the following is used for initial screening of auditory function in a neonate?
18 weeks pregnant female presents with no high risk of NTD and low risk of trisomy 21 on quad test. What is the most appropriate next step in management?
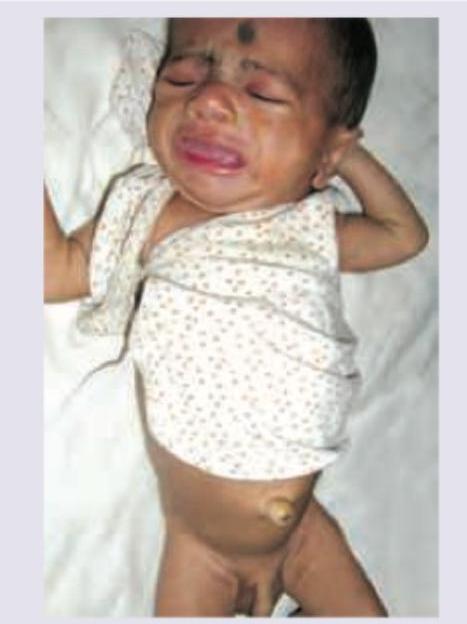
A neonate presents with the clinical features shown in the image below. What is the most likely diagnosis?
Consider the following disorders : 1. Delayed motor milestones 2. Spastic diplegia 3. Nyctalopia 4. Hearing defects Which of the above disorders occur as part of the spectrum of iodine deficiency disorders ?
The image shows a child with virilisation and clitoromegaly. What laboratory finding is typical for this condition, assuming the most common enzyme defect?
4 day old breastfed neonate, otherwise well, term neonate presented with jaundice, on testing the bilirubin level was found to be 18 mg/dl. Which of the following is the best step of management?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app