
V/Q scan principles — MCQs

A 50-year-old man presents to the urgent care clinic for 3 hours of worsening cough, shortness of breath, and dyspnea. He works as a long-haul truck driver, and he informs you that he recently returned to the west coast from a trip to Arkansas. His medical history is significant for gout, hypertension, hypercholesterolemia, diabetes mellitus type 2, chronic obstructive pulmonary disease (COPD), and mild intellectual disability. He currently smokes 1 pack of cigarettes/day, drinks a 6-pack of beer/day, and he endorses a past history of injection drug use but currently denies any illicit drug use. The vital signs include: temperature 36.7°C (98.0°F), blood pressure 126/74 mm Hg, heart rate 87/min, and respiratory rate 23/min. His physical examination shows mild, bilateral, coarse rhonchi, but otherwise clear lungs on auscultation, grade 2/6 holosystolic murmur, and a benign abdominal physical examination. He states that he ran out of his albuterol inhaler 6 days ago and has been meaning to follow-up with his primary care physician (PCP) for a refill. Complete blood count (CBC) and complete metabolic panel are within normal limits. He also has a D-dimer result within normal limits. Which of the following is the most appropriate next step in evaluation?
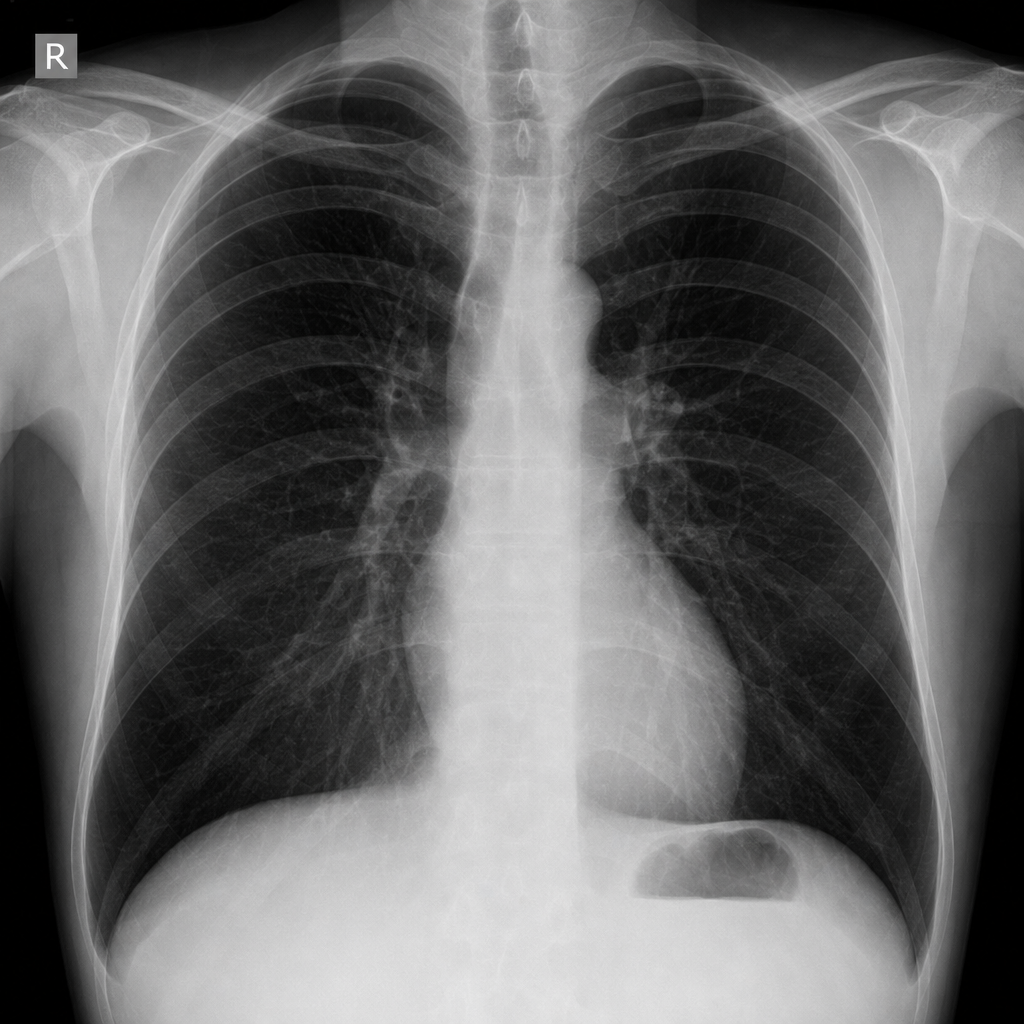
A 55-year-old man with a 60 pack-year smoking history is referred by his primary care physician for a pulmonary function test (PFT). A previously obtained chest x-ray is shown below. Which of the following will most likely appear in his PFT report?
A 60-year-old male is admitted to the ICU for severe hypertension complicated by a headache. The patient has a past medical history of insulin-controlled diabetes, hypertension, and hyperlipidemia. He smokes 2 packs of cigarettes per day. He states that he forgot to take his medications yesterday and started getting a headache about one hour ago. His vitals on admission are the following: blood pressure of 160/110 mmHg, pulse 95/min, temperature 98.6 deg F (37.2 deg C), and respirations 20/min. On exam, the patient has an audible abdominal bruit. After administration of antihypertensive medications, the patient has a blood pressure of 178/120 mmHg. The patient reports his headache has increased to a 10/10 pain level, that he has trouble seeing, and he can't move his extremities. After stabilizing the patient, what is the best next step to diagnose the patient's condition?
Four days after undergoing an elective total hip replacement, a 65-year-old woman develops a DVT that embolizes to the lung. Along with tachypnea, tachycardia, and cough, the patient would most likely present with a PaO2 of what?
A 71-year-old man presents to the emergency department for shortness of breath. The patient was returning from a business trip to China, when he suddenly felt short of breath during the taxi ride home from the airport. The patient has a past medical history of poorly controlled diabetes mellitus and a 50 pack-year smoking history. The patient is non-compliant with his medications and is currently only taking ibuprofen. An initial ECG demonstrates sinus tachycardia. A chest radiograph is within normal limits. Laboratory values are notable for a creatinine of 2.4 mg/dL and a BUN of 32 mg/dL as compared to his baseline creatinine of 0.9 mg/dL. His temperature is 98.8°F (37.1°C), pulse is 122/min, blood pressure is 145/90 mmHg, respirations are 19/min, and oxygen saturation is 93% on room air. On physical exam, you note an older gentleman in distress. Cardiac exam is notable only for tachycardia. Pulmonary exam is notable for expiratory wheezes. Which of the following is the best confirmatory test for this patient?
A 72-year-old man with coronary artery disease comes to the emergency department because of chest pain and shortness of breath for the past 3 hours. Troponin levels are elevated and an ECG shows ST-elevations in the precordial leads. Revascularization with percutaneous coronary intervention is performed, and a stent is successfully placed in the left anterior descending artery. Two days later, he complains of worsening shortness of breath. Pulse oximetry on 3L of nasal cannula shows an oxygen saturation of 89%. An x-ray of the chest shows distended pulmonary veins, small horizontal lines at the lung bases, and blunting of the costophrenic angles bilaterally. Which of the following findings would be most likely on a ventilation-perfusion scan of this patient?
During a clinical study examining the diffusion of gas between the alveolar compartment and the pulmonary capillary blood, men between the ages of 20 and 50 years are evaluated while they hold a sitting position. After inhaling a water-soluble gas that rapidly combines with hemoglobin, the concentration of the gas in the participant's exhaled air is measured and the diffusion capacity is calculated. Assuming that the concentration of the inhaled gas remains the same, which of the following is most likely to increase the flow of the gas across the alveolar membrane?
A 22-year-old man volunteers for a research study on lung function. He has no history of lung disease or allergies and does not smoke. His pulmonary blood flow is measured in the various labeled segments of the lungs while standing. Then the volunteer, still standing, is given very low continuous positive airway pressure and the blood flow measured again. Which of the following sets of findings are most likely to be present in the second measurements relative to the first?
A 57-year-old man presents to the clinic for a chronic cough over the past 4 months. The patient reports a productive yellow/green cough that is worse at night. He denies any significant precipitating event prior to his symptoms. He denies fever, chest pain, palpitations, weight changes, or abdominal pain, but endorses some difficulty breathing that waxes and wanes. He denies alcohol usage but endorses a 35 pack-year smoking history. A physical examination demonstrates mild wheezes, bibasilar crackles, and mild clubbing of his fingertips. A pulmonary function test is subsequently ordered, and partial results are shown below: Tidal volume: 500 mL Residual volume: 1700 mL Expiratory reserve volume: 1500 mL Inspiratory reserve volume: 3000 mL What is the functional residual capacity of this patient?
A 68-year-old man comes to the emergency room with difficulty in breathing. He was diagnosed with severe obstructive lung disease a few years back. He uses his medication but often has to come to the emergency room for intravenous therapy to help him breathe. He was a smoker for 40 years smoking two packs of cigarettes every day. Which of the following best represents the expected changes in his ventilation, perfusion and V/Q ratio?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app