
V/Q mismatch in COPD — MCQs

A 48-year-old man comes to the physician because of a 3-month history of worsening shortness of breath and cough productive of frothy, whitish sputum. One year ago, he had a similar episode lasting 6 months. He has smoked a pack of cigarettes daily for 25 years. Physical examination shows bluish discoloration of the tongue and lips. Scattered expiratory wheezing and rhonchi are heard throughout both lung fields. Further evaluation of this patient is most likely to show which of the following findings?
A 65-year-old woman presents to her physician with chronic breathlessness. Her condition has been progressively worsening over the last 20 years despite treatment with inhaled salbutamol, inhaled corticosteroids, and multiple courses of antibiotics. She has a 30-pack-year smoking history but quit 20 years ago. Her pulse is 104/min and respirations are 28/min. Physical examination shows generalized wasting. Chest auscultation reveals expiratory wheezes bilaterally and distant heart sounds. Pulmonary function testing shows a non-reversible obstructive pattern. Her carbon monoxide diffusion capacity of the lungs (DLCO) is markedly reduced. Which of the following explains the underlying mechanism of her condition?
A 22-year-old man volunteers for a research study on lung function. He has no history of lung disease or allergies and does not smoke. His pulmonary blood flow is measured in the various labeled segments of the lungs while standing. Then the volunteer, still standing, is given very low continuous positive airway pressure and the blood flow measured again. Which of the following sets of findings are most likely to be present in the second measurements relative to the first?
In which of the following pathological states would the oxygen content of the trachea resemble the oxygen content in the affected alveoli?
A 72-year-old obese man presents as a new patient to his primary care physician because he has been feeling tired and short of breath after recently moving to Denver. He is a former 50 pack-year smoker and has previously had deep venous thrombosis. Furthermore, he previously had a lobe of the lung removed due to lung cancer. Finally, he has a family history of a progressive restrictive lung disease. Laboratory values are obtained as follows: Oxygen tension in inspired air = 130 mmHg Alveolar carbon dioxide tension = 48 mmHg Arterial oxygen tension = 58 mmHg Respiratory exchange ratio = 0.80 Respiratory rate = 20/min Tidal volume = 500 mL Which of the following mechanisms is consistent with these values?
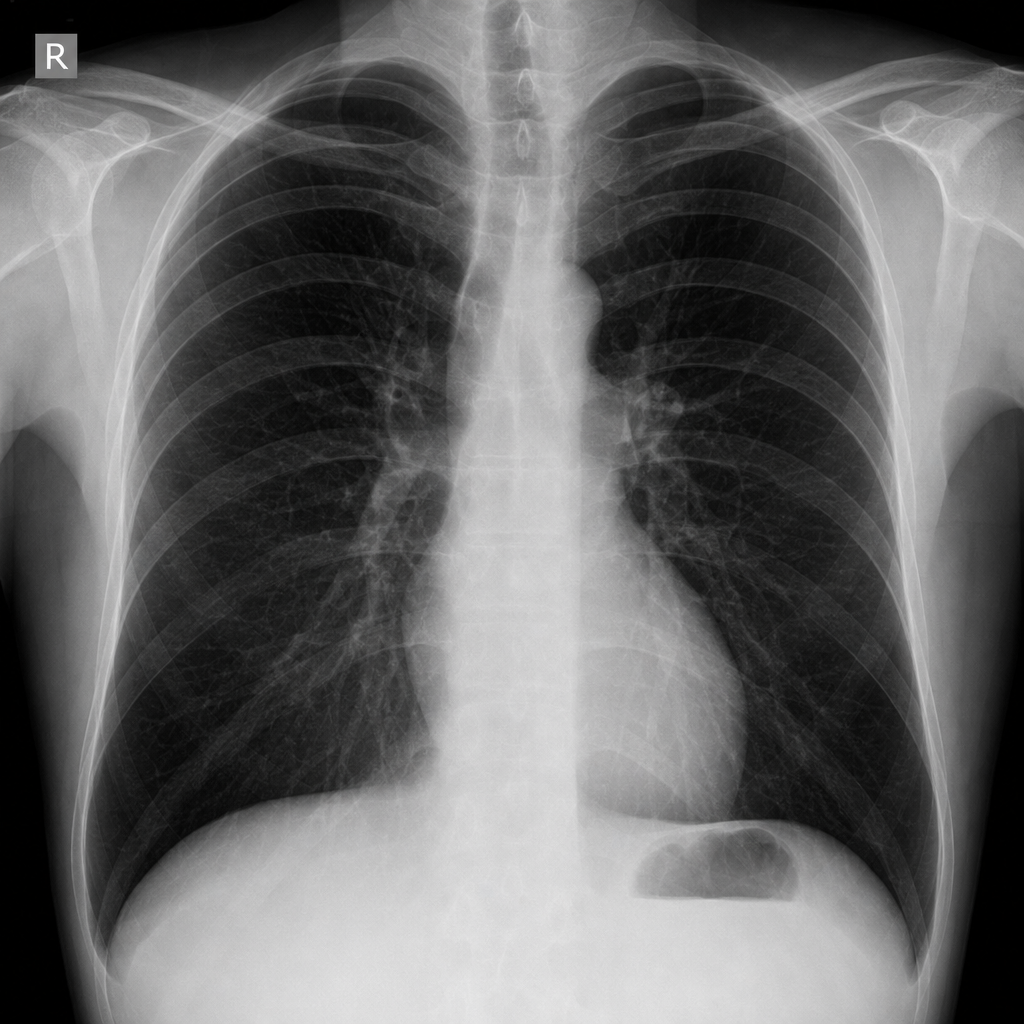
A 55-year-old man with a 60 pack-year smoking history is referred by his primary care physician for a pulmonary function test (PFT). A previously obtained chest x-ray is shown below. Which of the following will most likely appear in his PFT report?
Two days after undergoing left hemicolectomy for a colonic mass, a 62-year-old man develops shortness of breath. His temperature is 38.1°C (100.6°F), pulse is 80/min, respirations are 22/min, and blood pressure is 120/78 mm Hg. Pulse oximetry on room air shows an oxygen saturation of 88%. Cardiopulmonary examination shows decreased breath sounds and decreased fremitus at both lung bases. Arterial blood gas analysis on room air shows: pH 7.35 PaO2 70 mm Hg PCO2 40 mm Hg An x-ray of the chest shows a collapse of the bases of both lungs. Which of the following is the most likely underlying mechanism of this patient's hypoxemia?
A 64-year-old man presents to his primary care physician for follow-up of a severe, unrelenting, productive cough of 2 years duration. The medical history includes type 2 diabetes mellitus, which is well-controlled with insulin. He has a 25-pack-year smoking history and is an active smoker. The blood pressure is 135/88 mm Hg, the pulse is 94/min, the temperature is 36.9°C (98.5°F), and the respiratory rate is 18/min. Bilateral wheezes and crackles are heard on auscultation. A chest X-ray reveals cardiomegaly, increased lung markings, and a flattened diaphragm. Which of the following is most likely in this patient?
A 68-year-old man comes to the emergency room with difficulty in breathing. He was diagnosed with severe obstructive lung disease a few years back. He uses his medication but often has to come to the emergency room for intravenous therapy to help him breathe. He was a smoker for 40 years smoking two packs of cigarettes every day. Which of the following best represents the expected changes in his ventilation, perfusion and V/Q ratio?
A 62-year-old man is brought to the emergency department with a 2-day history of cough productive of yellowish sputum. He has had fever, chills, and worsening shortness of breath over this time. He has a 10-year history of hypertension and hyperlipidemia. He does not drink alcohol or smoke cigarettes. His current medications include atorvastatin, amlodipine, and metoprolol. His temperature is 38.9°C (102.0°F), pulse is 105/min, respirations are 27/min, and blood pressure is 110/70 mm Hg. He appears in mild distress. He has rales over the left lower lung field. The remainder of the examination shows no abnormalities. Leukocyte count is 15,000/mm3 (87% segmented neutrophils). Arterial blood gas analysis on room air shows: pH 7.44 pO2 68 mm Hg pCO2 28 mm Hg HCO3- 24 mEq/L O2 saturation 91% An x-ray of the chest shows a consolidation in the left lower lobe. Asking the patient to lie down in the left lateral decubitus position would most likely result in which of the following?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app