
V/Q mismatch — MCQs

On this page
A 62-year-old man is brought to the emergency department with a 2-day history of cough productive of yellowish sputum. He has had fever, chills, and worsening shortness of breath over this time. He has a 10-year history of hypertension and hyperlipidemia. He does not drink alcohol or smoke cigarettes. His current medications include atorvastatin, amlodipine, and metoprolol. His temperature is 38.9°C (102.0°F), pulse is 105/min, respirations are 27/min, and blood pressure is 110/70 mm Hg. He appears in mild distress. He has rales over the left lower lung field. The remainder of the examination shows no abnormalities. Leukocyte count is 15,000/mm3 (87% segmented neutrophils). Arterial blood gas analysis on room air shows: pH 7.44 pO2 68 mm Hg pCO2 28 mm Hg HCO3- 24 mEq/L O2 saturation 91% An x-ray of the chest shows a consolidation in the left lower lobe. Asking the patient to lie down in the left lateral decubitus position would most likely result in which of the following?
A 52-year-old woman presents to the emergency department with breathlessness for the past 6 hours. She denies cough, nasal congestion or discharge, sneezing, blood in sputum, or palpitation. There is no past history of chronic respiratory or cardiovascular medical conditions, but she mentions that she has been experiencing frequent cramps in her left leg for the past 5 days. She is post-menopausal and has been on hormone replacement therapy for a year now. Her temperature is 38.3°C (100.9°F), the pulse is 116/min, the blood pressure is 136/84 mm Hg, and the respiratory rate is 24/min. Edema and tenderness are present in her left calf region. Auscultation of the chest reveals rales over the left infrascapular and scapular region. The heart sounds are normal and there are no murmurs. Which of the following mechanisms most likely contributed to the pathophysiology of this patient’s condition?
A 22-year-old man volunteers for a research study on lung function. He has no history of lung disease or allergies and does not smoke. His pulmonary blood flow is measured in the various labeled segments of the lungs while standing. Then the volunteer, still standing, is given very low continuous positive airway pressure and the blood flow measured again. Which of the following sets of findings are most likely to be present in the second measurements relative to the first?
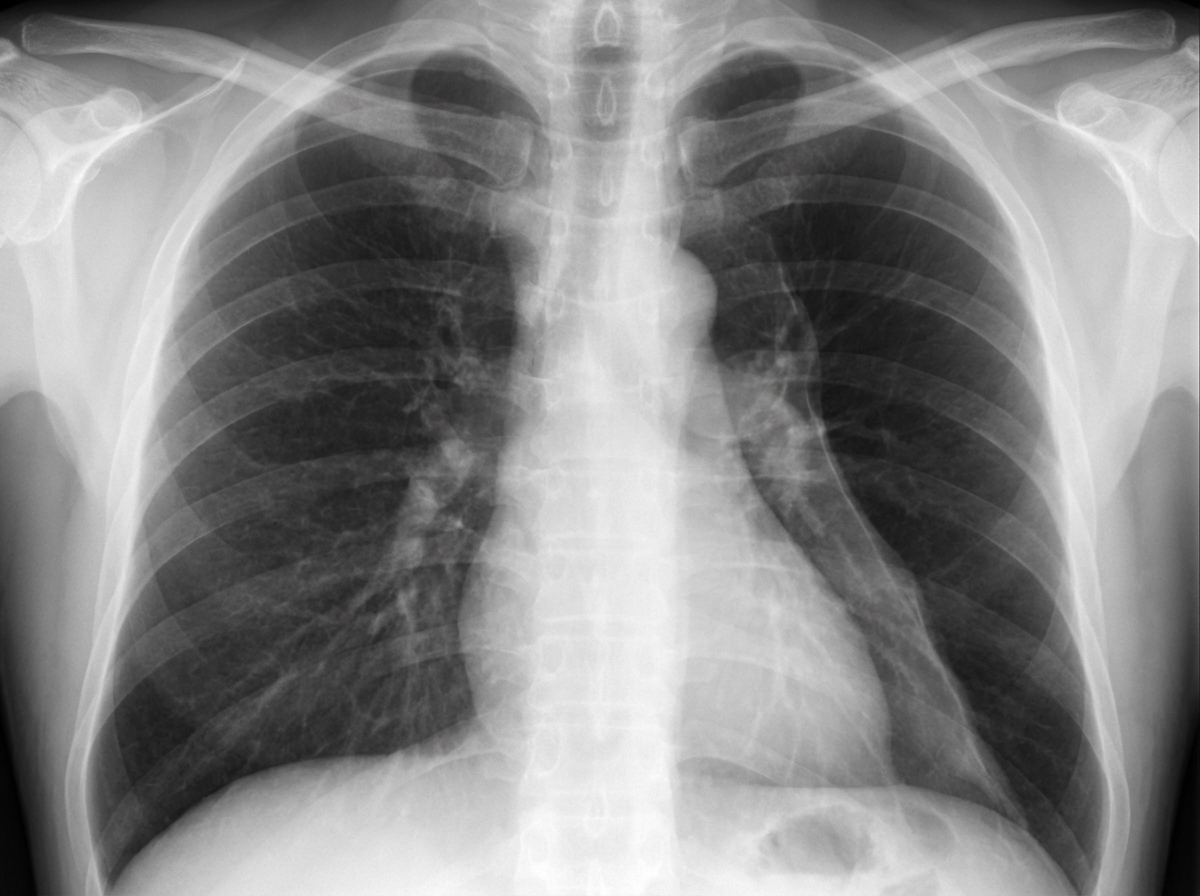
A 19-year-old man comes to the emergency department with sharp, left-sided chest pain and shortness of breath. He has no history of recent trauma. He does not smoke or use illicit drugs. He is 196 cm (6 feet 5 in) tall and weighs 70 kg (154 lb); BMI is 18 kg/m2. Examination shows reduced breath sounds over the left lung field. An x-ray of the chest is shown. Which of the following changes is most likely to immediately result from this patient's current condition?
A 17-year-old boy is brought to the physician by his father because of fever, congestion, and malaise for the past 2 days. He reports a sensation of pressure over his nose and cheeks. Over the past year, he has had an intermittent cough productive of green sputum and lately has noticed some streaks of blood in the sputum. He has had over 10 episodes of sinusitis, all of which were successfully treated with antibiotics. There is no family history of serious illness. The patient's vaccinations are up-to-date. His temperature is 38°C (100.4°F), pulse is 90/min, and blood pressure is 120/80 mm Hg. Physical examination shows tenderness to palpation over both cheeks. Crackles and rhonchi are heard on auscultation of the chest. Cardiac examination shows an absence of heart sounds along the left lower chest. Which of the following additional findings is most likely in this patient?
Practice by Chapter
Ventilation-perfusion ratio concept
Practice Questions
Normal V/Q distribution
Practice Questions
Alveolar dead space (high V/Q)
Practice Questions
Shunt physiology (low V/Q)
Practice Questions
Gravity effects on V/Q distribution
Practice Questions
V/Q ratio and gas exchange
Practice Questions
Hypoxic pulmonary vasoconstriction
Practice Questions
V/Q mismatch in COPD
Practice Questions
V/Q mismatch in pulmonary embolism
Practice Questions
V/Q mismatch in ARDS
Practice Questions
V/Q scan principles
Practice Questions
Oxygen therapy effects on V/Q mismatch
Practice Questions
Ventilator strategies addressing V/Q
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app