
Respiratory — MCQs

On this page
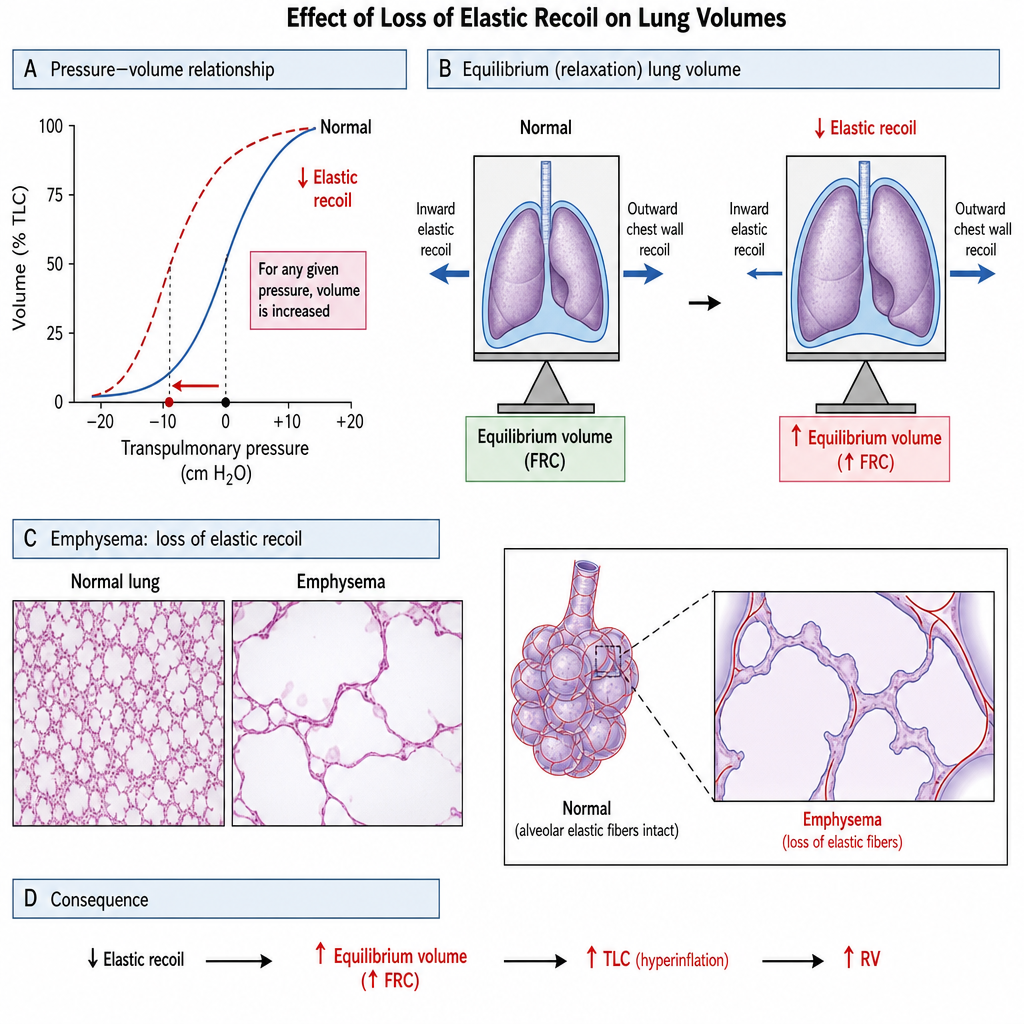
A 58-year-old man with a history of chronic obstructive pulmonary disease is evaluated in the pulmonary function laboratory. The FEV1 is 1.1 L, the FVC is 2.9 L, and the TLC is 7.8 L (predicted 6.0 L). After administration of an inhaled bronchodilator, FEV1 increases to 1.3 L and FVC increases to 3.1 L. Which of the following best characterizes the physiological basis of his increased TLC?
Practice by Chapter
Respiratory mechanics and work of breathing
Practice Questions
Pulmonary volumes and capacities
Practice Questions
Spirometry interpretation
Practice Questions
Flow-volume loops
Practice Questions
Airway resistance determinants
Practice Questions
Control of breathing
Practice Questions
Central and peripheral chemoreceptors
Practice Questions
Respiratory centers in the brainstem
Practice Questions
Exercise respiratory physiology
Practice Questions
Sleep effects on respiration
Practice Questions
High altitude adaptation
Practice Questions
Dyspnea mechanisms
Practice Questions
Integrated respiratory responses
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app