
Renal — MCQs

On this page
A 34-year-old man presents to his primary care physician with frequent urination. He was recently hospitalized following a severe motorcycle accident in which he suffered multiple injuries to his head and extremities. He reports that he has been constantly thirsty and has been urinating four to five times per night since being discharged from the hospital one week prior to presentation. His past medical history is notable for type II diabetes mellitus, which is well controlled on metformin. He has a 10 pack-year smoking history and drinks 3-4 alcoholic beverages per day. His temperature is 98.8°F (37.1°C), blood pressure is 110/70 mmHg, pulse is 95/min, and respirations are 18/min. Physical examination reveals delayed capillary refill and decreased skin turgor. Notable laboratory results are shown below: Serum: Na+: 148 mEq/L Cl-: 101 mEq/L K+: 3.7 mEq/L HCO3-: 25 mEq/L BUN: 20 mg/dL Glucose: 110 mg/dL Hemoglobin A1c: 5.7% This patient’s condition is most likely caused by defective production in which of the following locations?
Two days after undergoing an emergency laparotomy following a motor vehicle collision, a 37-year-old man has increased thirst. Examination shows dry mucous membranes and decreased skin turgor. A review of his chart shows his urine output to be in excess of his fluid intake. Laboratory studies show a serum sodium concentration of 151 mEq/L and urine osmolality of 110 mOsmol/kg H2O. One hour after the administration of desmopressin, the serum sodium concentration is 146 mEq/L and urine osmolality is 400 mOsmol/kg H2O. One week later, his laboratory values are within normal limits. This patient's condition was most likely caused by damage to which of the following structures?
A 45-year-old gentleman with a history of poorly controlled diabetes mellitus is referred to a nephrologist for evaluation of the possibility of early stage kidney failure. Upon evaluation, the nephrologist decides to assess the patient's renal plasma flow by performing a laboratory test. Which of the following substances would be the best for estimating this value?
A 46-year-old African American woman presents to her primary care doctor complaining of muscle aches and weakness. She reports a 3 month history of gradually worsening upper and lower extremity pain. She is having trouble keeping up with her children and feels tired for most of the day. A review of systems reveals mild constipation. Her past medical history is notable for hypertension, diabetes, rheumatoid arthritis, and obesity. She takes lisinopril, metformin, and methotrexate. Her family history is notable for chronic lymphocytic leukemia in her mother and prostate cancer in her father. Her temperature is 99°F (37.2°C), blood pressure is 145/95 mmHg, pulse is 80/min, and respirations are 17/min. On exam, she appears well and in no acute distress. Muscle strength is 4/5 in her upper and lower extremities bilaterally. Patellar and brachioradialis reflexes are 2+ bilaterally. A serum analysis in this patient would most likely reveal which of the following?
A researcher is studying gamete production and oogenesis. For her experiment, she decides to cultivate primary oocytes in their arrested state and secondary oocytes just prior to fertilization. When she examines these gametes, she will find that the primary oocytes and secondary oocytes are arrested in which phases of meiosis, respectively?
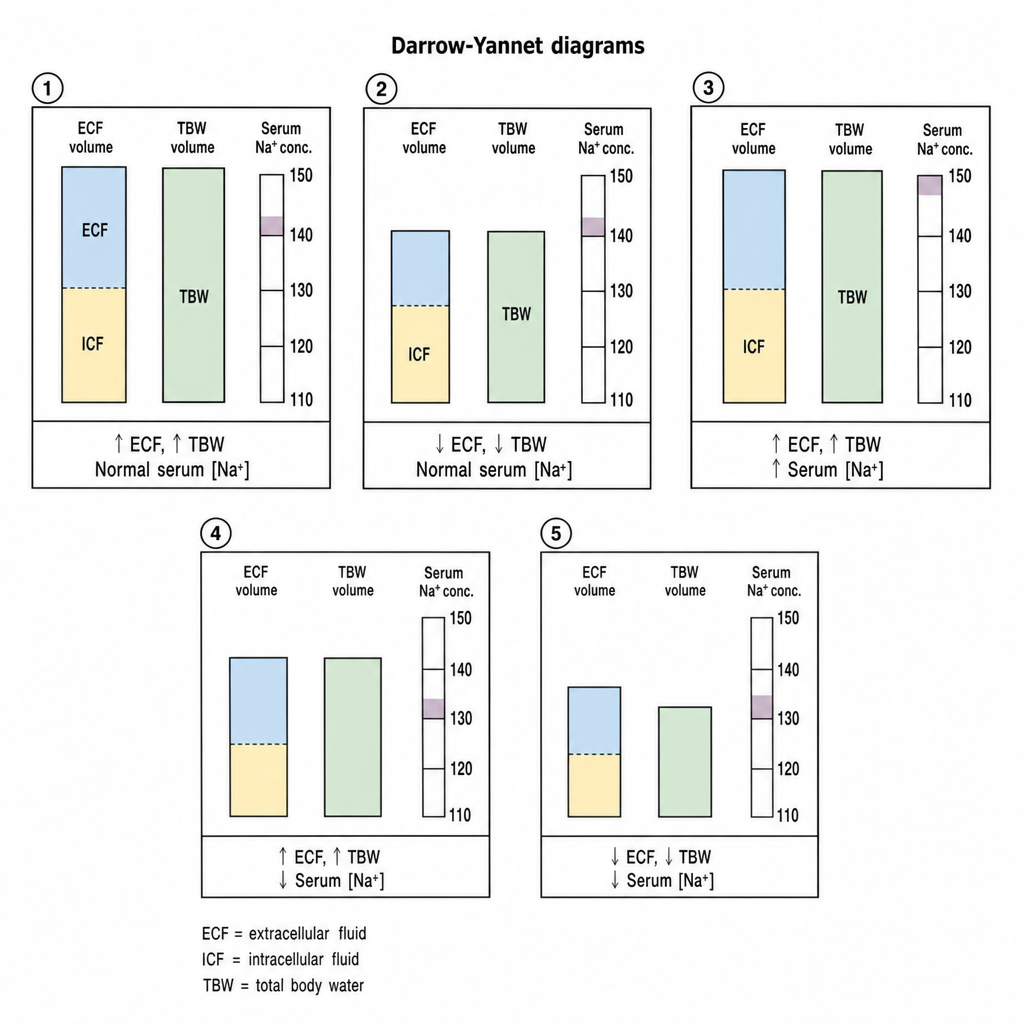
A 28-year-old man presents to his physician with a history of excessive thirst and excessive urination over the last 3 weeks. He mentions that he has to wake up multiple times at night to urinate. A detailed history reveals that he has a known case of bipolar mood disorder and has been taking lithium carbonate for 5 years. His urinary specific gravity is 1.003, and his urinary osmolality is 150 mOsm/kg H2O. Which of the following Darrow-Yannet diagrams best describes the status of volumes and osmolality of this man’s body fluids?
A 53-year-old woman with endometriosis comes to the physician because of bilateral flank pain and decreased urine output for 1-week. She has not had any fevers, chills, or dysuria. Physical examination shows several surgical scars on her abdomen. Laboratory studies show a serum creatinine concentration of 3.5 mg/dL. A CT scan of the abdomen shows numerous intra-abdominal adhesions, as well as dilatation of the renal pelvis and proximal ureters bilaterally. An increase in which of following is the most likely underlying mechanism of this patient's renal dysfunction?
A 65-year-old female with chronic renal failure presents with recent onset of bone pain. Serum analysis reveals decreased levels of calcium and elevated levels of parathyroid hormone. One of the mechanisms driving the elevated PTH is most similar to that seen in:
A 17-year-old girl comes to the physician because of a 12-hour history of profuse watery diarrhea with flecks of mucus that started shortly after she returned from a trip to South America. She has not had any fever or nausea. Pulse is 104/min and blood pressure is 110/65 mm Hg. Physical examination shows dry mucous membranes and decreased skin turgor. Stool culture shows gram-negative, comma-shaped, flagellated bacilli. Therapy with oral rehydration solution is initiated. Which of the following is the most likely mechanism of this patient's diarrhea?
A 36-year-old man presents with the complaint of loose and watery stools for the past 3 days. He is now having bowel movements four to five times a day. He denies any blood or mucus in the stool. He also complains of abdominal pain and fatigue. Furthermore, he feels nauseous and does not feel like drinking anything. His urine is visibly yellow and low in volume. He recently returned from a trip to South America where he enjoyed all the local delicacies. He is most concerned about his urine color and volume. Which segment of the nephron is primarily responsible for these changes?
Practice by Chapter
Renal blood flow distribution
Practice Questions
Proximal tubule reabsorption
Practice Questions
Loop of Henle function
Practice Questions
Distal tubule and collecting duct function
Practice Questions
Concentration and dilution of urine
Practice Questions
Countercurrent multiplication system
Practice Questions
Sodium handling along the nephron
Practice Questions
Potassium balance and regulation
Practice Questions
Calcium and phosphate handling
Practice Questions
Magnesium handling
Practice Questions
Water balance and osmoregulation
Practice Questions
Diuretic mechanisms of action
Practice Questions
Integrated nephron function
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app