
Renal — MCQs

On this page
Following passage of a calcium oxalate stone, a 55-year-old male visits his physician to learn about nephrolithiasis prevention. Which of the following changes affecting urine composition within the bladder are most likely to protect against crystal precipitation?
A 64-year-old female presents to her primary care physician for an annual checkup. She states that her health is adequate, but she has not been doing well since her husband died last year. She is able to get by but admits to having trouble caring for herself, cooking, cleaning, and paying her bills. The patient complains of diffuse muscle aches and pains. She has a past medical history of anxiety and seasonal affective disorder. She is not currently taking any medications. On physical exam, you note a gaunt woman with a depressed affect. You note that her body mass index (BMI) and height have both decreased since her last annual visit. On physical exam, her cardiac, pulmonary, and abdominal exams are within normal limits. Lab work is drawn and is as follows: Serum: Na+: 135 mEq/L K+: 3.7 mEq/L Cl-: 100 mEq/L HCO3-: 23 mEq/L Urea nitrogen: 7 mg/dL Glucose: 70 mg/dL Creatinine: 0.8 mg/dL Ca2+: 8.0 mg/dL Mg2+: 1.5 mEq/L Parathyroid hormone: 855 pg/mL Alkaline phosphatase: 135 U/L Phosphorus: 2.6 mg/dL Hemoglobin: 14 g/dL Hematocrit: 36% Platelet count: 187,000/mm^3 Leukocyte count: 4,700/mm^3 What is the most likely diagnosis?
A 57-year-old male is found to have an elevated prostate specific antigen (PSA) level on screening labwork. PSA may be elevated in prostate cancer, benign prostatic hypertrophy (BPH), or prostatitis. Which of the following best describes the physiologic function of PSA?
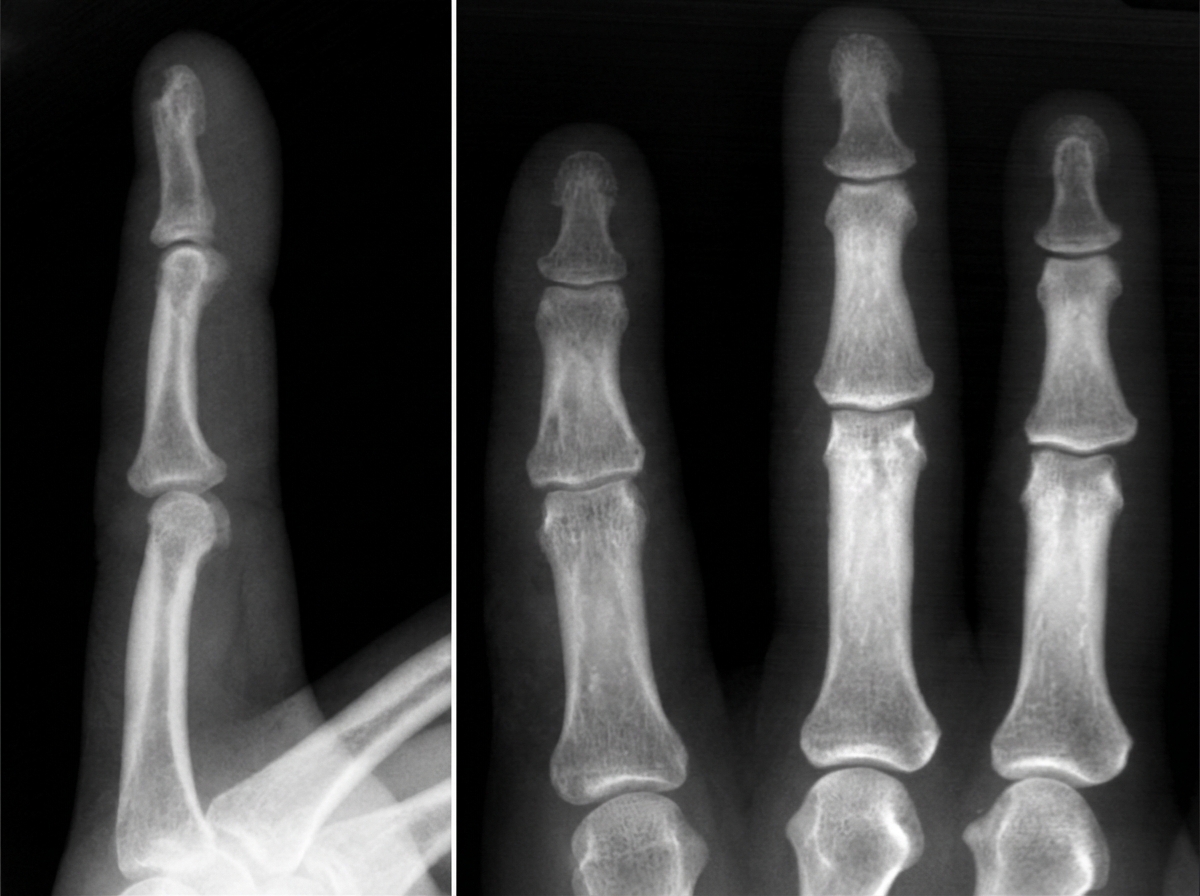
A 76-year-old woman presents to the office with a generalized weakness for the past month. She has a past medical history significant for uncontrolled hypertension and type 2 diabetes mellitus. Her temperature is 37.0°C (98.6°F), blood pressure is 135/82 mm Hg, pulse is 90/min, respiratory rate is 17/min, and oxygen saturation is 99% on room air. Physical exam shows no remarkable findings. Her last recorded glomerular filtration rate was 30 mL/min. A radiograph of the patient’s hand is given. Which of the following lab findings is most likely to be found in this patient?
A 23-year-old man presents to the office complaining of weight loss and fatigue for the past 2 months. He states that he has been experiencing foul-smelling, light-colored stools but thinks it is because he hasn’t been eating well, recently. He has a past medical history significant for cystic fibrosis, which is well-controlled medically. He denies any shortness of breath, chest or abdominal pain, nausea, vomiting, or melena. On physical examination, his skin is pale and dry. Which of the following would be the most likely etiology of a malabsorption syndrome giving rise to this patient’s current condition?
A healthy 30-year-old female has a measured creatinine clearance of 100 mL/min. She has a filtration fraction (FF) of 25%. Serum analysis reveals a creatinine level of 0.9 mg/dL and an elevated hematocrit of 0.6. Which of the following is the best estimate of this patient’s renal blood flow?
In a healthy patient with no renal abnormalities, several mechanisms are responsible for moving various filtered substances into and out of the tubules. Para-aminohippurate (PAH) is frequently used to estimate renal blood flow when maintained at low plasma concentrations. The following table illustrates the effect of changing plasma PAH concentrations on PAH excretion: Plasma PAH concentration (mg/dL) | Urinary PAH concentration (mg/dL) 0 | 0 10 | 60 20 | 120 30 | 150 40 | 180 Which of the following mechanisms best explains the decreased rate of increase in PAH excretion observed when plasma PAH concentration exceeds 20 mg/dL?
A 10-year-old boy is brought to a pediatric clinic by his parents with pain and weakness in the lower extremities for the past 3 weeks. The patient’s mother says that he has been active until the weakness and pain started during his soccer practice sessions. He says he also experiences muscle cramps, especially at night. His mother adds that, recently, the patient constantly wakes up in the night to urinate and is noticeably thirsty most of the time. The patient denies any recent history of trauma to his legs. His vaccinations are up to date and his family history is unremarkable. His vital signs are within normal limits. Physical examination is unremarkable. Laboratory findings are shown below: Laboratory test Serum potassium 3.3 mEq/L Serum magnesium 1.3 mEq/L Serum chloride 101 mEq/L pH 7.50 Pco2 38 mm Hg HCO3- 20 mEq/L Po2 88 mm Hg Which of the following is the most likely diagnosis in this patient?
A 42-year-old man is brought to the emergency room because of confusion. His wife says he has been urinating more frequently than usual for the past 3 days. He has not had fever or dysuria. He has bipolar disorder, for which he takes lithium. His pulse is 105/min, and respirations are 14/min. He is lethargic and oriented only to person. Physical examination shows dry mucous membranes and increased capillary refill time. Laboratory studies show a serum sodium concentration of 158 mEq/L and an antidiuretic hormone (ADH) concentration of 8 pg/mL (N = 1–5). Which of the following is the most likely site of dysfunction in this patient?
An investigator is studying physiologic renal responses to common medical conditions. She measures urine osmolalities in different parts of the nephron of a human subject in the emergency department. The following values are obtained: Portion of nephron Osmolality (mOsmol/kg) Proximal convoluted tubule 300 Loop of Henle, descending limb 1200 Loop of Henle, ascending limb 250 Distal convoluted tubule 100 Collecting duct 1200 These values were most likely obtained from an individual with which of the following condition?
Practice by Chapter
Renal blood flow distribution
Practice Questions
Proximal tubule reabsorption
Practice Questions
Loop of Henle function
Practice Questions
Distal tubule and collecting duct function
Practice Questions
Concentration and dilution of urine
Practice Questions
Countercurrent multiplication system
Practice Questions
Sodium handling along the nephron
Practice Questions
Potassium balance and regulation
Practice Questions
Calcium and phosphate handling
Practice Questions
Magnesium handling
Practice Questions
Water balance and osmoregulation
Practice Questions
Diuretic mechanisms of action
Practice Questions
Integrated nephron function
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app