
Distal tubule and collecting duct function — MCQs

A 61-year-old male is given acetazolamide to treat open-angle glaucoma. Upon diuresis, his urine is found to be highly alkaline. Which of the following accounts for the alkaline nature of this patient’s urine?
An investigator is studying patients with acute decompensated congestive heart failure. He takes measurements of a hormone released from atrial myocytes, as well as serial measurements of left atrial and left ventricular pressures. The investigator observes a positive correlation between left atrial pressures and the serum level of this hormone. Which of the following is most likely the mechanism of action of this hormone?
A 54-year-old woman comes to the physician for a follow-up examination after presenting with elevated blood pressure readings during her last two visits. After her last visit 2 months ago, she tried controlling her hypertension with weight loss before starting medical therapy, but she has since been unable to lose any weight. Her pulse is 76/min, and blood pressure is 154/90 mm Hg on the right arm and 155/93 mm Hg on the left arm. She agrees to start treatment with a thiazide diuretic. In response to this treatment, which of the following is most likely to decrease?
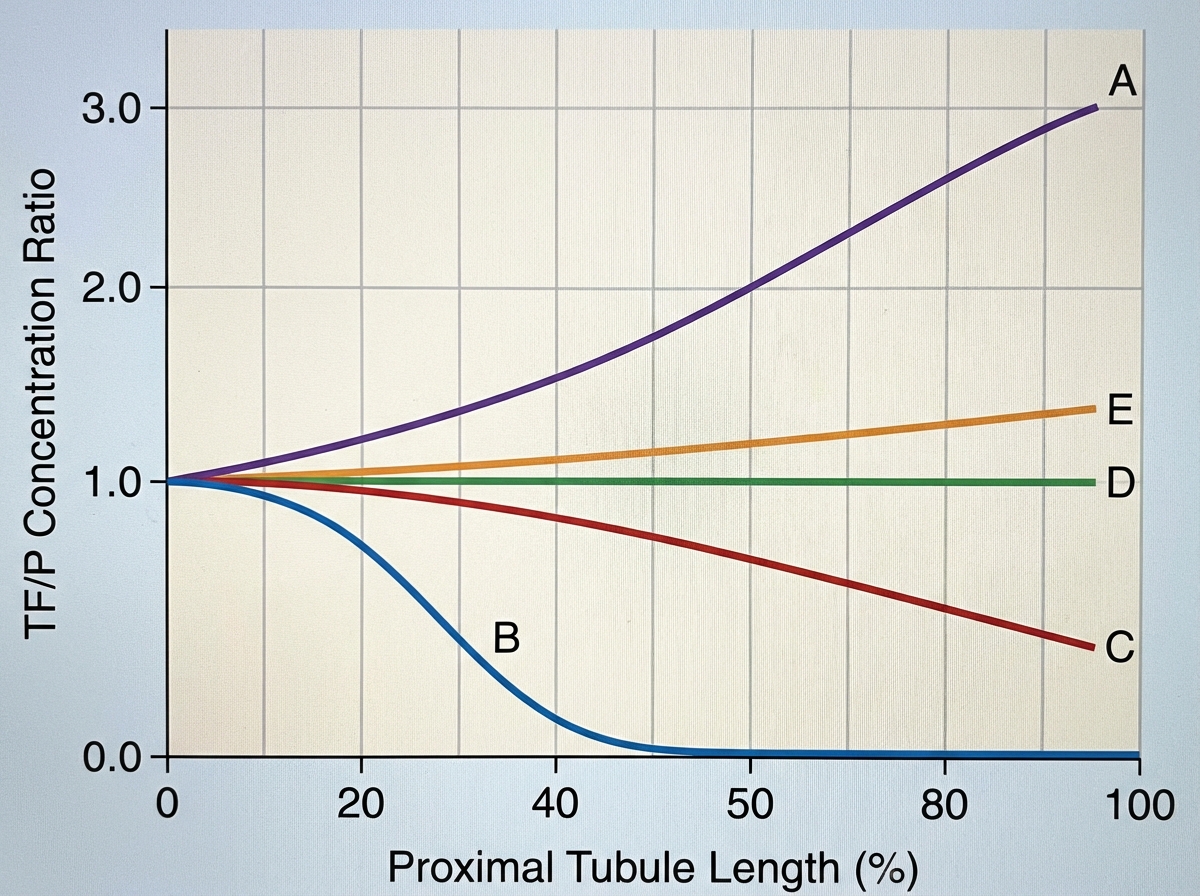
A 72-year-old female is brought to the emergency department after being found unresponsive in her garage with an open bottle of unmarked fluid. She is confused and is unable to answer questions on arrival. Her medical history is significant for Alzheimer disease, but her family says she has no medical comorbidities. Serum analysis of this patient's blood shows a pH of 7.28 with a high anion gap. The electrolyte that is most likely significantly decreased in this patient follows which of the following concentration curves across the proximal tubule of the kidney?
A researcher is studying the effects of a new antihypertensive medication on urine osmolality. She first measures urine osmolality in different parts of the nephron of a healthy human control. The findings are shown below: Portion of nephron Urine osmolality (mOsmol/kg) Proximal convoluted tubule 300 Loop of Henle, descending limb 1200 Loop of Henle, ascending limb 200 Distal convoluted tubule 100 Collecting duct 600 Which of the following is the most likely explanation for the urine osmolality in the ascending limb of the loop of Henle?
On cardiology service rounds, your team sees a patient admitted with an acute congestive heart failure exacerbation. In congestive heart failure, decreased cardiac function leads to decreased renal perfusion, which eventually leads to excess volume retention. To test your knowledge of physiology, your attending asks you which segment of the nephron is responsible for the majority of water absorption. Which of the following is a correct pairing of the segment of the nephron that reabsorbs the majority of all filtered water with the means by which that segment absorbs water?
A new drug X is being tested for its effect on renal function. During the experiments, the researchers found that in patients taking substance X, the urinary concentration of sodium decreases while urine potassium concentration increase. Which of the following affects the kidneys in the same way as does substance X?
A 55-year-old woman presents to the emergency room with severe abdominal pain for the past 24 hours. She has also noticed blood in her urine. She does not have any significant past medical history. Family history is significant for her mother having cholecystitis status post cholecystectomy at age 45. Her vital signs include: temperature 36.8°C (98.2°F), pulse 103/min, respiratory rate 15/min, blood pressure 105/85 mm Hg. Physical examination is significant for a woman continuously moving on the exam table in an attempt to get comfortable. Laboratory findings are significant for the following: Serum electrolytes Na 138 mEq/L N: 135–145 mEq/L K 4.0 mEq/L N: 3.5–5.0 mEq/L Cl 102 mEq/L N: 98–108 mEq/L CO2 27 mEq/L N: 22–32 mEq/L Ca 9.2 mEq/dL N: 8.4–10.2 mEq/dL PO4 3.5 mg/dL N: 3.0–4.5 mg/dL A 24-hour urine collection is performed and reveals a urinary calcium of 345 mg/day (ref: < 300 mg/day in men; < 250 mg/day in women). A non-contrast CT of the abdomen is performed and is shown in the exhibit. The patient’s symptoms pass within the next 12 hours with hydration and acetaminophen for pain management. She is prescribed a medication to prevent subsequent episodes. At which of the following parts of the nephron does this medication most likely work?

A 17-year-old boy is brought to the physician by his father because of a 7-month history of fatigue, recurrent leg cramps, and increased urinary frequency. His pulse is 94/min and blood pressure is 118/85 mm Hg. Physical examination shows dry mucous membranes. Laboratory studies show: Serum Na+ 130 mEq/L K+ 2.8 mEq/L Cl- 92 mEq/L Mg2+ 1.1 mEq/L Ca2+ 10.6 mg/dL Albumin 5.2 g/dL Urine Ca2+ 70 mg/24 h Cl- 375 mEq/24h (N = 110–250) Arterial blood gas analysis on room air shows a pH of 7.55 and an HCO3- concentration of 45 mEq/L. Impaired function of which of the following structures is the most likely cause of this patient's condition?
A 57-year-old male is found to have an elevated prostate specific antigen (PSA) level on screening labwork. PSA may be elevated in prostate cancer, benign prostatic hypertrophy (BPH), or prostatitis. Which of the following best describes the physiologic function of PSA?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app